Criteria for the Diagnosis of Microvascular Inflammation (MVI) in Kidney Transplant Biopsies (KTxBx).
1Dept. of Lab Medicine &
Pathology, Mayo Clinic College of Medicine, Rochester, MN
2Division of Biostatistics, U. Minnesota School of Public Health, Minneapolis, MN.
Meeting: 2016 American Transplant Congress
Abstract number: 121
Keywords: Alloantibodies, Biopsy, Graft survival, Histology
Session Information
Session Name: Concurrent Session: Kidney AMR: Making the Diagnosis
Session Type: Concurrent Session
Date: Sunday, June 12, 2016
Session Time: 4:30pm-6:00pm
 Presentation Time: 5:06pm-5:18pm
Presentation Time: 5:06pm-5:18pm
Location: Veterans Auditorium
The presence of MVI (Banff glomerulitis "g" score and Banff peritubular capillary "ptc" score) in KTxBx, often related to antibody mediated rejection (AMR), is associated with reduced graft survival and is one of three Banff criteria needed for a diagnosis of AMR. However neither the current minimal Banff criteria for a diagnosis of MVI nor the impact of varying degrees of MVI have been validated in a large patient population.
The objective of this study was to define the impact of MVI among 478 patients biopsied due to new onset kidney graft dysfunction (25% increase in Scr or new onset proteinuria) ≥ 3 months after transplant enrolled in the two Long-term Deterioration of Kidney Allograft Function (DeKAF) Study cohorts (cross sectional (CSC): 229 patients; prospective (PC): 249 patients). Biopsies showing other potential causes of graft dysfunction – recurrent glomerulonephritis, BK nephropathy, and transplant glomerulopathy – were excluded. Biopsies were read centrally by a single pathologist (JG) and graded in strict accordance with Banff criteria. Impact of MVI was assessed by the hazard ratio (HR) for death censored graft failure. Initial analyses examined the impact of ptc ≥ 1, g ≥ 1, or both, compared with absence of both ptc and g (111, 18, 63, and 286 patients respectively). The HR for any g or ptc score ≥ 1 compared with both = 0 were similar (HR: 2.1 and 2.7 respectively). To evaluate the impact of higher scores of either g or ptc, a composite score for MVI (MVI score) totaling the individual ptc and g scores was determined. As shown in the figure, graft loss was significantly more frequent with any MVI score > 0 than with an MVI score = 0 [HRs 2.8 – 3.7, all p < 0.0001], but outcomes at each score > 0 were virtually identical (all comparisons p > 0.14). The impact of MVI was not different between biopsies in the CSC and PC cohorts.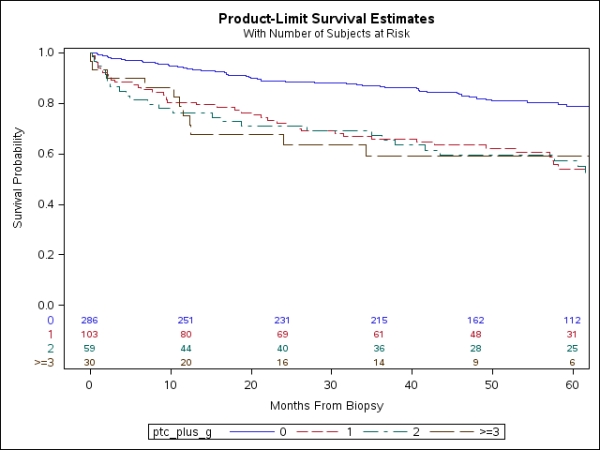
We conclude that MVI should be diagnosed in the presence of any Banff ptc or g score > 0, and that the impact of MVI on death censored kidney graft failure is independent of total MVI score > 0.
CITATION INFORMATION: Grande J, Leduc R, The DeKAF Study Group Criteria for the Diagnosis of Microvascular Inflammation (MVI) in Kidney Transplant Biopsies (KTxBx). Am J Transplant. 2016;16 (suppl 3).
To cite this abstract in AMA style:
Grande J, Leduc R, Group TheDeKAFStudy. Criteria for the Diagnosis of Microvascular Inflammation (MVI) in Kidney Transplant Biopsies (KTxBx). [abstract]. Am J Transplant. 2016; 16 (suppl 3). https://atcmeetingabstracts.com/abstract/criteria-for-the-diagnosis-of-microvascular-inflammation-mvi-in-kidney-transplant-biopsies-ktxbx/. Accessed May 17, 2026.« Back to 2016 American Transplant Congress