Use of a CMV Specific T Cell Immunity Assay in Late-Onset CMV Infection
1Department of Internal Medicine - Division Infectious Diseases, UCLA, Los Angeles, CA, 2Department of Internal Medicine - Division Nephrology, UCLA, Los Angeles, CA
Meeting: 2019 American Transplant Congress
Abstract number: A321
Keywords: Cytomeglovirus, Kidney/liver transplantation, Prophylaxis, T cell reactivity
Session Information
Session Name: Poster Session A: Transplant Infectious Diseases
Session Type: Poster Session
Date: Saturday, June 1, 2019
Session Time: 5:30pm-7:30pm
 Presentation Time: 5:30pm-7:30pm
Presentation Time: 5:30pm-7:30pm
Location: Hall C & D
*Purpose: To describe our clinical experience using a CMV Specific Cell Mediated Immunity (CMI) assay in solid organ transplant (SOT) recipients with late-onset CMV, defined as CMV infection occurring after discontinuation of routine prophylaxis.
*Methods: SOT recipients with CMV infection underwent testing for CMV specific CMI (CMV T Cell Immunity Panel, Viracor Eurofins Laboratories) at the discretion of their treating Infectious Diseases clinicians.
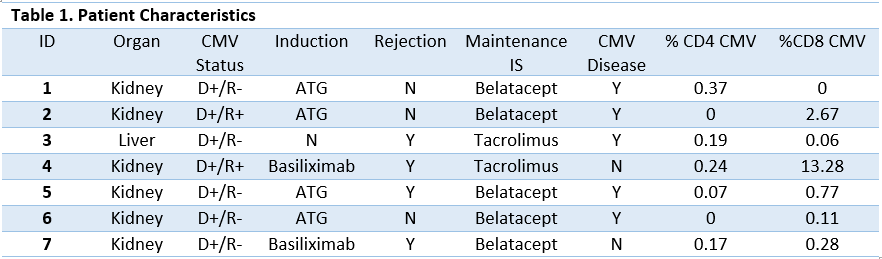
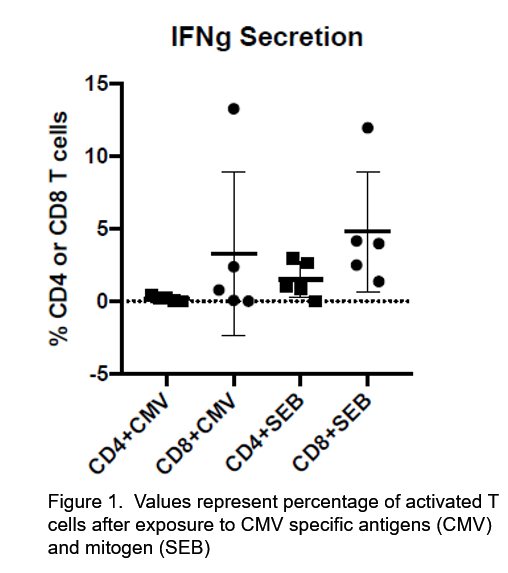
*Results: Patient characteristics are noted in table 1. 5/7 had CMV mismatch, 4/7 received ATG and 5/7 had belatacept as part of their maintenance immunosuppressive (IS) regimen at time of CMV onset. All had late-onset CMV infection after completing post-transplant prophylaxis with valganciclovir (VGCV), median onset 64 days from stopping (range 34 – 175). 5/7 had CMV disease. CMV CMI assay results are in figure 1. Only one (4) had initial CMV CD4 and CD8 response > 0.2% (0.2% is the manufacturer validated cut-off for healthy adults); 4/7 had appropriate response to SEB stimulation (positive control). On average, CD8 response was higher than CD4. 4/7 have follow-up CMV CMI assay results available. Patient 4 had CD4 and CD8 response > 0.2% on initial and follow-up testing and remains aviremic 2 months off secondary prophylaxis. One patient (5) had interval development of CMV CMI on follow-up. Initial CD4 and CD8 CMV responses were 0.07% and 0.77% respectively; on repeat testing 8 weeks later CD4 and CD8 response had increased to 0.6% and 1.76%. In the setting of highly resistant CMV they were maintained on letermovir as secondary prophylaxis for planned 3-months. The other 2 patients with follow-up testing (3 & 6) had substandard CMI responses on follow-up and have been maintained on secondary prophylaxis.
*Conclusions: New IS regimens may contribute to impaired development of effective CMV-specific CMI in high risk patients who are at risk for late-onset CMV disease. Measurement of CMV specific CMI is a potential approach for identifying patients with ongoing risk for late CMV disease who may benefit from prolonged surveillance or use of antiviral prophylaxis.
To cite this abstract in AMA style:
Beaird O, Carlson M, Gaynor P, Nanayakkara D, Abdalla B, Bunnapradist S, Schaenman J. Use of a CMV Specific T Cell Immunity Assay in Late-Onset CMV Infection [abstract]. Am J Transplant. 2019; 19 (suppl 3). https://atcmeetingabstracts.com/abstract/use-of-a-cmv-specific-t-cell-immunity-assay-in-late-onset-cmv-infection/. Accessed June 3, 2026.« Back to 2019 American Transplant Congress