Unexpected Early Calcineurin Inhibitor Nephrotoxicity in Pediatric Kidney Transplant Recipients.
1Pediatrics, University of Alabama at Birmingham, Birmingham, AL
2Medicine, University of Alabama at Birmingham, Birmingham, AL.
Meeting: 2016 American Transplant Congress
Abstract number: D157
Keywords: Biopsy, Graft function, Kidney transplantation, Nephrotoxicity
Session Information
Session Name: Poster Session D: Kidney-Pediatrics
Session Type: Poster Session
Date: Tuesday, June 14, 2016
Session Time: 6:00pm-7:00pm
 Presentation Time: 6:00pm-7:00pm
Presentation Time: 6:00pm-7:00pm
Location: Halls C&D
Background: Calcineurin inhibitors effectively suppress the recipient immune response and facilitate early success in kidney transplantation. However, these drugs are potent nephrotoxins and contribute to late allograft loss in adults. The contribution of calcineurin inhibitor nephrotoxicity (CNIT) to pediatric graft dysfunction is unknown.
Objective: To analyze a large single-center cohort of pediatric kidney transplant recipients (KTRs), assess the frequency of and risk factors for early CNIT, and determine the impact on long term outcomes.
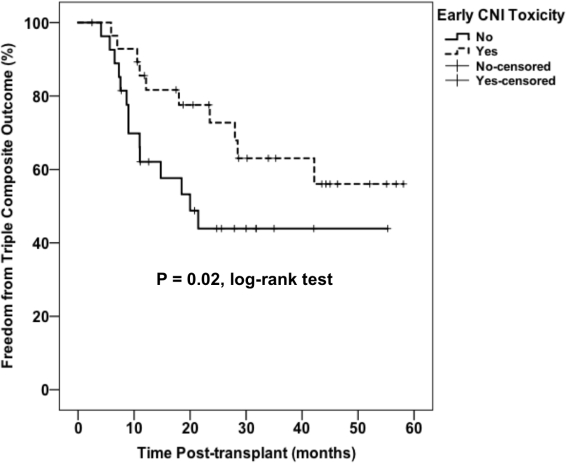
Methods: We retrospectively reviewed surveillance and indication biopsies performed within 6 months of transplant at our center between Aug 2008 to Dec 2014. CNIT was defined as biopsy evidence of striped fibrosis, arteriolar hyalinosis, tubular vacuolization, or pathologist interpretation of drug effect. First we explored risk factors associated with early CNIT. Second we evaluated a composite outcome of death, graft loss, and T cell mediated rejection based on early CNIT. Secondary outcomes were estimated GFR (eGFR) at 1 year and last follow up. Chi square, t tests, and Kaplan-Meier methods were used for data analysis.
Results: The cohort included 75 subjects with a median age at biopsy of 12 years. African Americans (AAs) comprised 50% of our cohort. Early CNIT occurred in 37 patients (49%). Patients with early CNIT were more likely to be AA (68% in CNIT vs 34% in no CNIT, p=0.004), but there were no significant differences in age, gender, donor type, or early non-adherence. There were no significant differences in eGFR between patients with vs without early CNIT. After adjusting for race, those with early CNIT had lower incidence of the composite outcome (p=0.02, see figure).
Conclusions: Early CNIT was highly prevalent in pediatric KTRs, especially AA recipients, but had no effect on early graft function. Patients with early CNIT had lower incidence of death, graft loss, or rejection, which suggests reversibility of early CNIT and supports the potency of CNI-based regiments in children.
CITATION INFORMATION: Yanik M, Mannon R, Seifert M. Unexpected Early Calcineurin Inhibitor Nephrotoxicity in Pediatric Kidney Transplant Recipients. Am J Transplant. 2016;16 (suppl 3).
To cite this abstract in AMA style:
Yanik M, Mannon R, Seifert M. Unexpected Early Calcineurin Inhibitor Nephrotoxicity in Pediatric Kidney Transplant Recipients. [abstract]. Am J Transplant. 2016; 16 (suppl 3). https://atcmeetingabstracts.com/abstract/unexpected-early-calcineurin-inhibitor-nephrotoxicity-in-pediatric-kidney-transplant-recipients/. Accessed May 27, 2026.« Back to 2016 American Transplant Congress