Treatment of BK Virus with Weekly Intravenous Immunoglobulin in Adult Kidney Transplant Recipients
1Department of Pharmacy, Yale New Haven Hospital, New Haven, CT, 2Section of Nephrology, Yale School of Medicine, New Haven, CT
Meeting: 2022 American Transplant Congress
Abstract number: 1355
Keywords: Infection, IVIG, Kidney transplantation, Polyma virus
Topic: Clinical Science » Infection Disease » 26 - Kidney: Polyoma
Session Information
Session Time: 7:00pm-8:00pm
 Presentation Time: 7:00pm-8:00pm
Presentation Time: 7:00pm-8:00pm
Location: Hynes Halls C & D
*Purpose: The typical management of Polyoma BK virus (BKV) in kidney transplant recipients (KTR) includes reducing immunosuppression (IS). Intravenous immunoglobulin (IVIG) has been utilized for BKV management with various dosing strategies. This report reviews the use of 0.1 g/kg weekly of IVIG as treatment for persistent BKV.
*Methods: This retrospective chart review included all adult KTR at Yale New Haven Hospital with BKV receiving IVIG 0.1 g/kg weekly for 10 weeks. All patients previously underwent reduction of maintenance IS without clearance of BKV. Those receiving any other IVIG dosing strategy and or with <6 month follow-up were excluded. Persistent BKV was defined as PCR >3 Log10 copies/mL despite IS reduction. Clearance was defined as undetectable viral load or <3 Log10 copies/mL . Patient demographics, BKV log10, and serum creatinine (SCr) were collected at 3 and 6 months. Rates of biopsy proven rejection (BPAR) and graft loss were also collected.
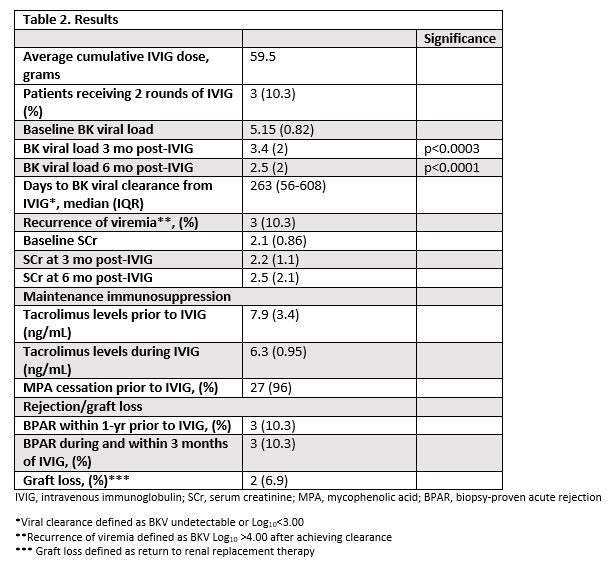
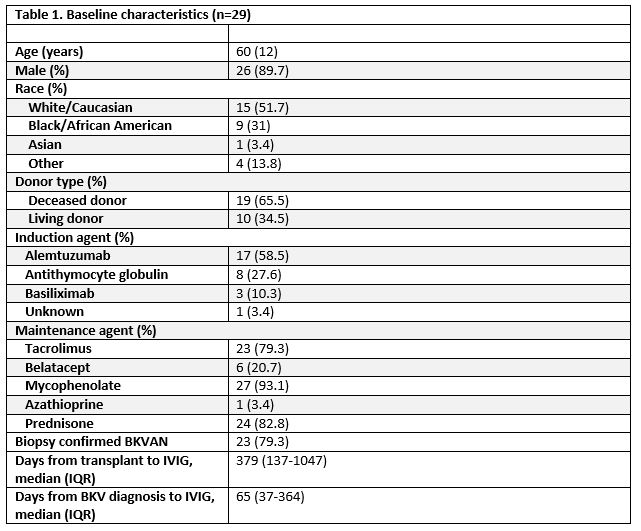
*Results: 29 adult KTR with BKV who received IVIG 0.1 g/kg weekly for 10 weeks were included. The majority of patients were received alemtuzumab induction (58.6%), were on a tacrolimus (79.3%) and were a median of 379 (137-1047) days from transplant. BKV-associated nephropathy was biopsy confirmed in 79.3%. The average cumulative amount of IVIG given was 59.5 g. Mycophenolic acid (MPA) was stopped prior to IVIG in 96% of patients. There was a significant reduction in average BKV log10 from baseline to 3 months (5.15 vs. 3.14, p<0.0003) and 6 months post-IVIG (5.15 vs. 2.47, p<0.0001). Viral clearance occurred in 65% of patients at a median of 263 days (IQR 56-608) from last IVIG. Only 1 patient was changed to everolimus during IVIG, and no other alternative BKV treatments were utilized. BPAR occurred in 3 patients after starting IVIG and graft loss in 2 patients.
*Conclusions: Treatment of BKV with IVIG 0.1 g/kg weekly for 10 weeks without additional alternative therapies provided a significant reduction in BK viral log10 at 3 and 6 months post IVIG in KTR with persistent BKV despite reduction in IS. Further comparative studies are needed however this review highlights the potential efficacy of weekly IVIG in KTR not on additional anti-virals.
To cite this abstract in AMA style:
Girone G, Asch W. Treatment of BK Virus with Weekly Intravenous Immunoglobulin in Adult Kidney Transplant Recipients [abstract]. Am J Transplant. 2022; 22 (suppl 3). https://atcmeetingabstracts.com/abstract/treatment-of-bk-virus-with-weekly-intravenous-immunoglobulin-in-adult-kidney-transplant-recipients/. Accessed May 27, 2026.« Back to 2022 American Transplant Congress