Significance of Detectable but Unquantifiable Viremias Post Renal Transplantation
Robert Wood Johnson University Hospital, New Brunswick, NJ
Meeting: 2021 American Transplant Congress
Abstract number: 804
Keywords: Cytomeglovirus, Kidney transplantation, Kidney/pancreas transplantation, Polyma virus
Topic: Clinical Science » Infectious Disease » Kidney: Polyoma
Session Information
Session Name: Kidney: Polyoma
Session Type: Poster Abstract
Session Date & Time: None. Available on demand.
Location: Virtual
*Purpose: It is unknown whether the degree of the initial viremia following kidney (KT) or combined kidney-pancreas transplantation (SPKT) correlates with future allograft rejection or loss. We sought to characterize transplant outcomes based on initial BK virus and cytomegalovirus (CMV) level.
*Methods: In this single center, retrospective, observational study 97 adult KT (88%)/SPKT (12%) recipients (age>18 years old) transplanted from 2018-2019 with first detectable CMV and BK viremia during their first year of transplant were included. Adults with BK or CMV viremia were divided into groups based on whether their initial PCR results were quantifiable (QL, Group1) or only detectable (DL, Group2). The primary end-points were biopsy proven acute rejection and graft loss following initial treatment for BK or CMV viremia. Initial treatment of BK viremia or CMV viremia was defined as any immunosuppression (IS) reduction (for BK viremia > 2000 copies/ml and CMV level >500 copies/ml).
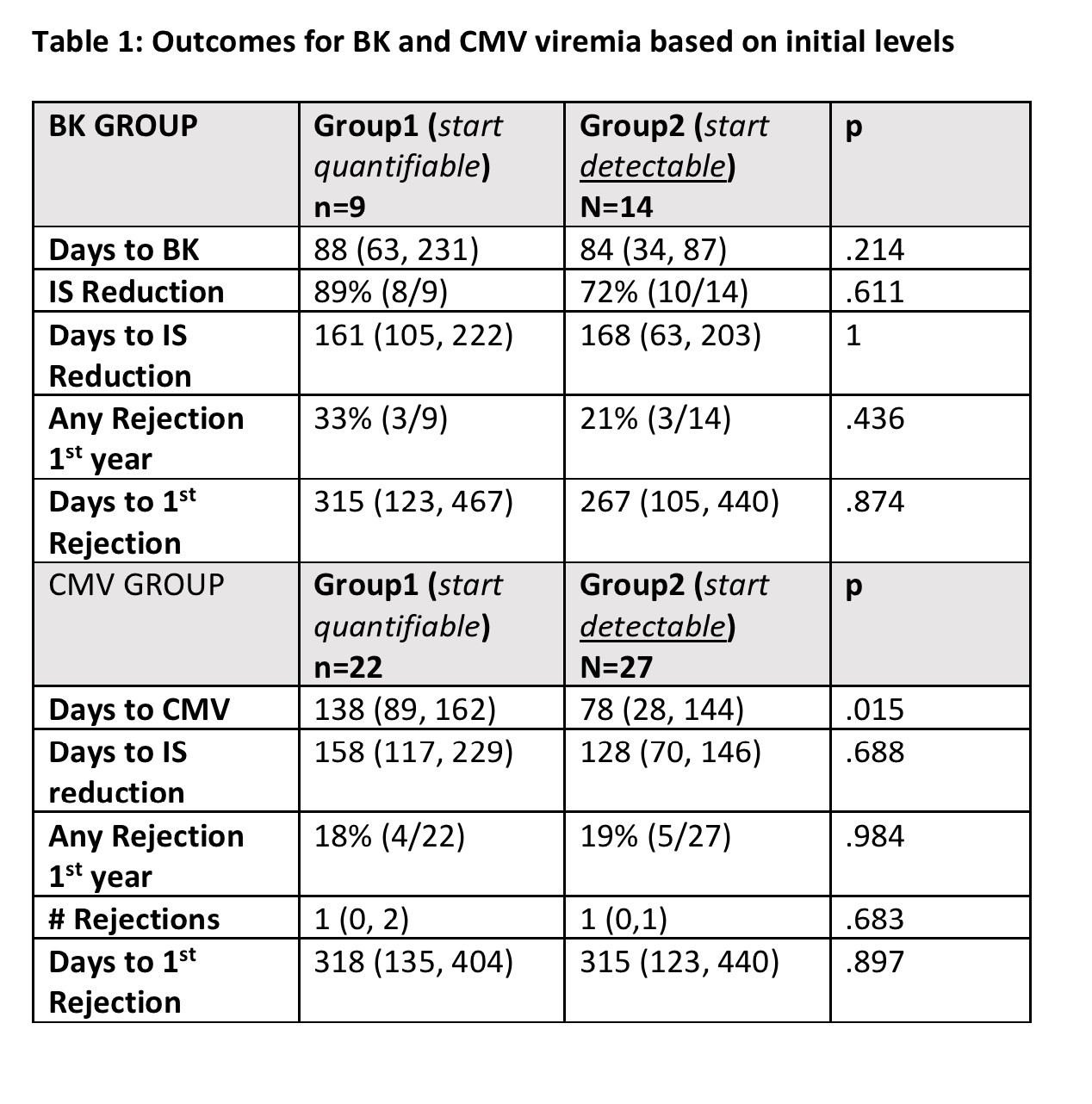
*Results: Demographics: Males (52%), Blacks (35%), deceased donor (68%) and thymoglobulin induction (97%). There were no differences in donor or recipient demographics between BK or CMV categories when comparing initial detectable (DL) and quantifiable (QL) groupings. Using detectability as the threshold, the incidences of BK and CMV in the first 6 months were 19% (18/97) and 41% (40/97) respectively. The median time to rejection overall was 214 (96, 373) days. 12/13 (92%) of those patients had a concurrent BK or CMV viremia. A viremia preceded a rejection in 5/6 cases with BK and 7/10 cases with CMV. Comparing DL and QL groupings, for BK/CMV there were no differences in primary end points, days to viremia, days to treatment, and percentage of patients requiring viremia targeted therapy (Table 1). 50% of BK and 40% of CMV patients with initial DL never progressed to QL.
*Conclusions: Initial viremia for both BK and CMV does not seem to correlate disease severity or post-transplant outcomes.
To cite this abstract in AMA style:
Chaung M, Puri S, Bunin S, Mondal Z, Eletta O, Pelletier R, Bongu A. Significance of Detectable but Unquantifiable Viremias Post Renal Transplantation [abstract]. Am J Transplant. 2021; 21 (suppl 3). https://atcmeetingabstracts.com/abstract/significance-of-detectable-but-unquantifiable-viremias-post-renal-transplantation/. Accessed May 22, 2026.« Back to 2021 American Transplant Congress