Predictive Model of Delayed Graft Function in Machine Perfused Kidney Transplantation: Model Validation Using Decision Curve Analysis.
1Surgery, Duke University, Durham, NC
2Half Moon Bay, Raleigh.
Meeting: 2016 American Transplant Congress
Abstract number: C175
Keywords: Graft function, Kidney transplantation, Machine preservation, Outcome
Session Information
Session Name: Poster Session C: Kidney Transplantation: AKI/Preservation/DCD
Session Type: Poster Session
Date: Monday, June 13, 2016
Session Time: 6:00pm-7:00pm
 Presentation Time: 6:00pm-7:00pm
Presentation Time: 6:00pm-7:00pm
Location: Halls C&D
Introduction: Predictive model for delayed graft function (DGF) was developed (Am J Transpl 2010; 10: 2279–86)excluding organs that were machine perfused (MP). Currently, approximately 50% of organs are pumped. Given the evolution of MP, we aimed to refine the previously model (cold storage [CS] model) using recent data in MP organs.
Methods: The MP DGF risk model was developed using OPTN/UNOS data on, adult, non-preemptive, solitary, deceased donor renal transplants (2009 and 2013). Multivariable logistic regression model was fit to the data (n=18,648). The model was validated using a dataset of patients transplanted in 2014 (n=4,263). Calibration was assessed using the Hosmer-Lemeshow lack of fit (LoF) statistic. Clinical utility was evaluated using decision curve analysis (Med Decis Making 2006; 26:565-574). For comparison, the clinical utility of the CS model in MP organs was evaluated.
Results: Incidence of DGF between 2009 (27.6%) and 2014 (28.6%) remained constant. Overall predictive accuracy of the model was 73% (LoF = 9.86; p=0.275 on 8 df). Decision curve for the MP versus CS DGF risk model is depicted in Figure 1. DGF threshold probability of 30%, the net benefit of the MP model is 0.101 (Figure 1). This is equivalent to identifying 10 additional true-positive results per 100 patients without an increase in the number of false-positive results. Moreover, at a threshold probability of 30%, the net benefit of the DGF model is 0.115 greater than assuming all patients have DGF (Net Benefit: 0.101 – (-0.014)). This is equivalent to identifying 27 fewer false-positive results per 100 patients (Figure 2).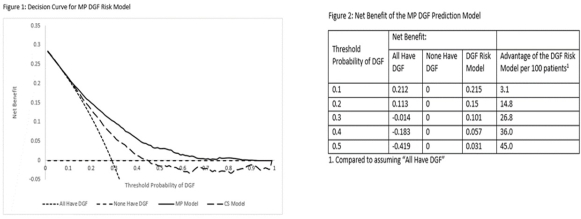
Conclusion: The MP DGF model is valid and well calibrated. Clinical utility was established using decision curve analysis across a wide range of DGF probability thresholds. At a DGF threshold probability of 30%, which is the current rate of DGF in MP organs, the DGF prediction model would identify 10 additional true-positive patients with DGF with 27 fewer false-positives per 100 patients. The enhanced ability will enable interventions to mitigate effects of DGF.
CITATION INFORMATION: Ravindra K, Sanoff S, Vikraman D, Patel U, Ellis M, Squires E, Sudan D, Irish W. Predictive Model of Delayed Graft Function in Machine Perfused Kidney Transplantation: Model Validation Using Decision Curve Analysis. Am J Transplant. 2016;16 (suppl 3).
To cite this abstract in AMA style:
Ravindra K, Sanoff S, Vikraman D, Patel U, Ellis M, Squires E, Sudan D, Irish W. Predictive Model of Delayed Graft Function in Machine Perfused Kidney Transplantation: Model Validation Using Decision Curve Analysis. [abstract]. Am J Transplant. 2016; 16 (suppl 3). https://atcmeetingabstracts.com/abstract/predictive-model-of-delayed-graft-function-in-machine-perfused-kidney-transplantation-model-validation-using-decision-curve-analysis/. Accessed May 21, 2026.« Back to 2016 American Transplant Congress