Predicting Immunologic Risk for Acute Rejection in Pediatric Liver Transplantation.
Yale University, New Haven, CT
Meeting: 2017 American Transplant Congress
Abstract number: 77
Keywords: HLA antibodies, Liver transplantation, Rejection
Session Information
Session Name: Concurrent Session: Pediatric Liver
Session Type: Concurrent Session
Date: Sunday, April 30, 2017
Session Time: 2:30pm-4:00pm
 Presentation Time: 2:54pm-3:06pm
Presentation Time: 2:54pm-3:06pm
Location: E271a
Background: Studies in heart, lung, kidney, & liver transplantation (LT) indicate an increased negative impact of antibodies (Ab) to HLA on allograft outcome.
Aim: To describe the frequency & timing of anti-HLA donor specific antibody (DSA) appearance following pediatric LT & the association between the presence of anti-HLA DSA & T-cell mediated rejection (ACR), viral infection, autoAb, & number of HLA antigen (Ag) mismatches.
Methods: Patients followed at our center from 7/31/98-2/29/16 were included (n=63). Anti-HLA DSA was screened in 42 LT recipients. DSA MFI >1000 was considered positive & evaluated retrospectively for ACR.
Results: 22 developed anti-HLA Class II DSA;20 did not  Those with Class II DSA had a higher rate of ACR (63.1% vs. 26.6%; p=0.03)
Those with Class II DSA had a higher rate of ACR (63.1% vs. 26.6%; p=0.03)
| DSA Class II: Yes | DSA Class II: No | p value | ||
| Any enzymes elevated | Yes | 14 (63.63 %) | 16 (80 %) | 0.39 |
| No | 8 (36.36 %) | 4 (20 %) | ||
| EBV | Yes | 5 (27.78 %) | 3 (21.43 %) | 1.00 |
| No | 13 (72.22 %) | 11 (78.57 %) | ||
| ACR on liver pathology | Yes | 12 (63.16 %) | 4 (26.67 %) | 0.034 |
| No | 7 (36.84 %) | 11 (73.33 %) | ||
| Any autoAb present | Yes | 5 (31.25 %) | 3 (25 %) | 1.00 |
| No | 11 (68.75 %) | 9 (75%) |
Rejection episodes coincided with DSA detection. Recipients with DQ Ag mismatches were less likely to have anti-smooth muscle Ab (4.76% vs. 75%; p=0.007). DSA appeared relatively early at 6-12 months post transplant 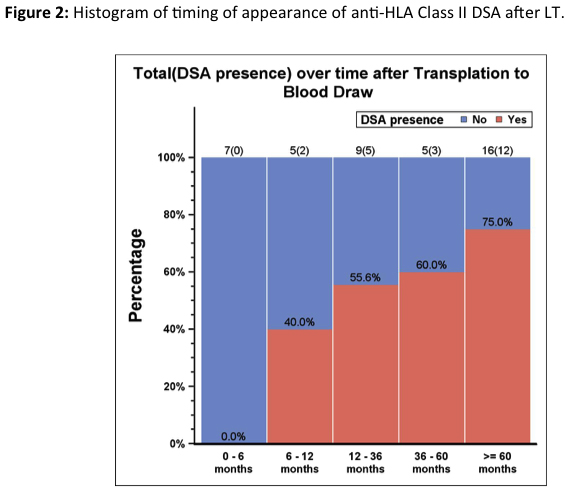 DQ Ag mismatch was not significantly associated with Class II DSA or ACR.
DQ Ag mismatch was not significantly associated with Class II DSA or ACR.
Conclusion: Ab-mediated mechanisms targeting HLA Ag may trigger immune responses like ACR. DQ Ag mismatch is not significantly correlated with ACR or de novo autoimmune hepatitis.
CITATION INFORMATION: Antala S, Bow L, Morotti R, Gan G, Yanhong D, Ekong U, Emre S. Predicting Immunologic Risk for Acute Rejection in Pediatric Liver Transplantation. Am J Transplant. 2017;17 (suppl 3).
To cite this abstract in AMA style:
Antala S, Bow L, Morotti R, Gan G, Yanhong D, Ekong U, Emre S. Predicting Immunologic Risk for Acute Rejection in Pediatric Liver Transplantation. [abstract]. Am J Transplant. 2017; 17 (suppl 3). https://atcmeetingabstracts.com/abstract/predicting-immunologic-risk-for-acute-rejection-in-pediatric-liver-transplantation/. Accessed May 16, 2026.« Back to 2017 American Transplant Congress