Poor Prognosis of Proliferative Glomerulonephritis with Monoclonal IgG Deposits in Renal Allografts: A Retrospective Multicenter Study from China
1National Clinical Research Center of Kidney Diseases, Jinling Hospital,Nanjing University Jinling School of Medicine, Nanjing, China, 2Department of Urology, Institute of Urology, West China Hospital, Sichuan University, Chengdu, China, 3Department of Urology, Henan Provincial People's Hospital
Zhengzhou University People's Hospital, Zhengzhou, China
Meeting: 2022 American Transplant Congress
Abstract number: 846
Keywords: Graft failure, IgG, Kidney transplantation, Prognosis
Topic: Clinical Science » Kidney » 47 - Kidney Complications: Immune Mediated Late Graft Failure
Session Information
Session Name: Kidney Complications: Immune Mediated Late Graft Failure
Session Type: Poster Abstract
Date: Saturday, June 4, 2022
Session Time: 5:30pm-7:00pm
 Presentation Time: 5:30pm-7:00pm
Presentation Time: 5:30pm-7:00pm
Location: Hynes Halls C & D
*Purpose: To analyze the clinicopathological characteristics, treatment efficacy and prognosis of proliferative glomerulonephritis with monoclonal IgG deposits (PGNMID) in renal allografts from multi-centers in China.
*Methods: We enrolled PGNMID cases confirmed by allograft biopsy from 8 hospitals in China from January 2005 to December 2019, then the clinical and laboratory data were collected and the risk factors associated with prognosis were analyzed in all enrolled cases.
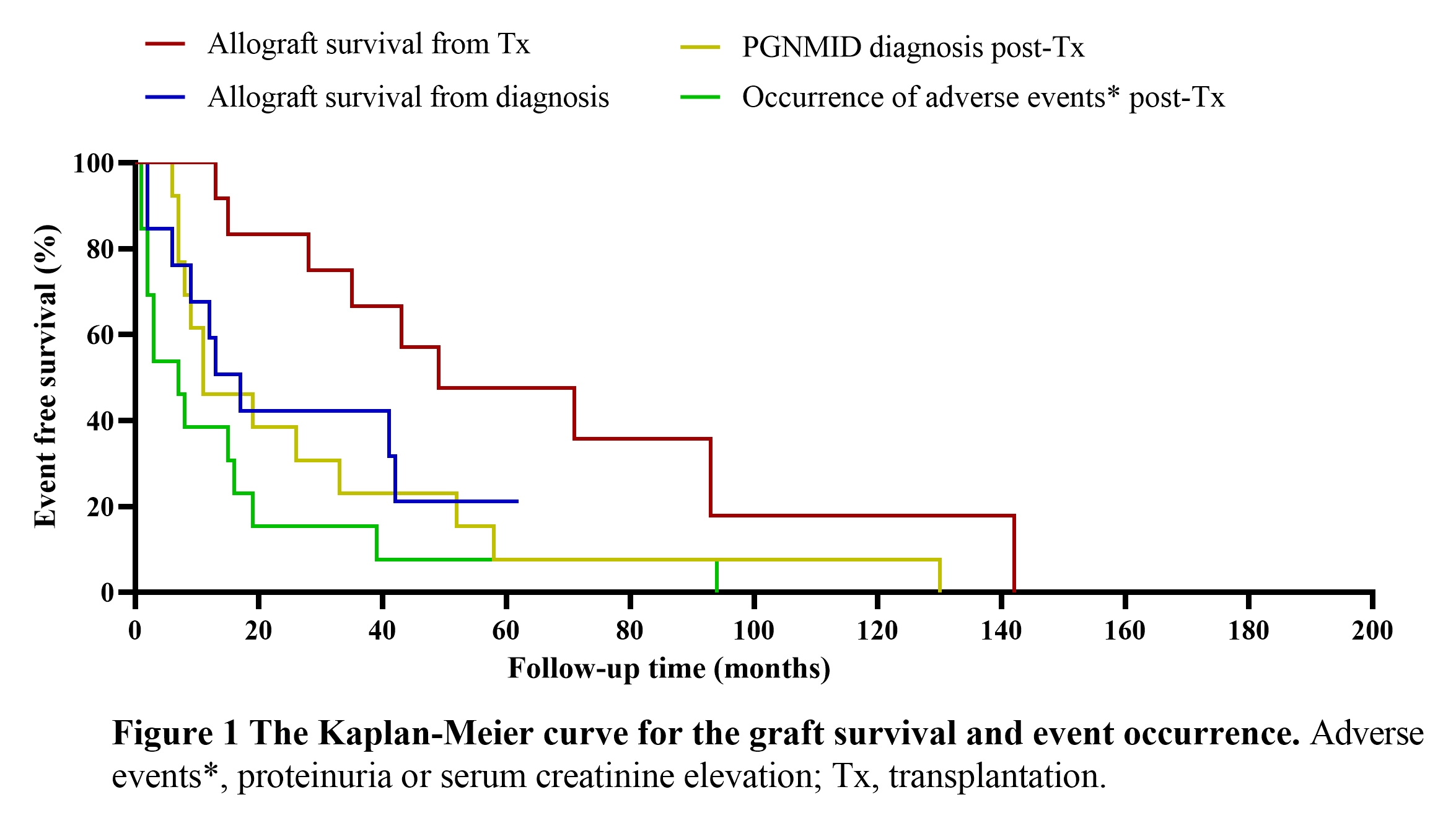
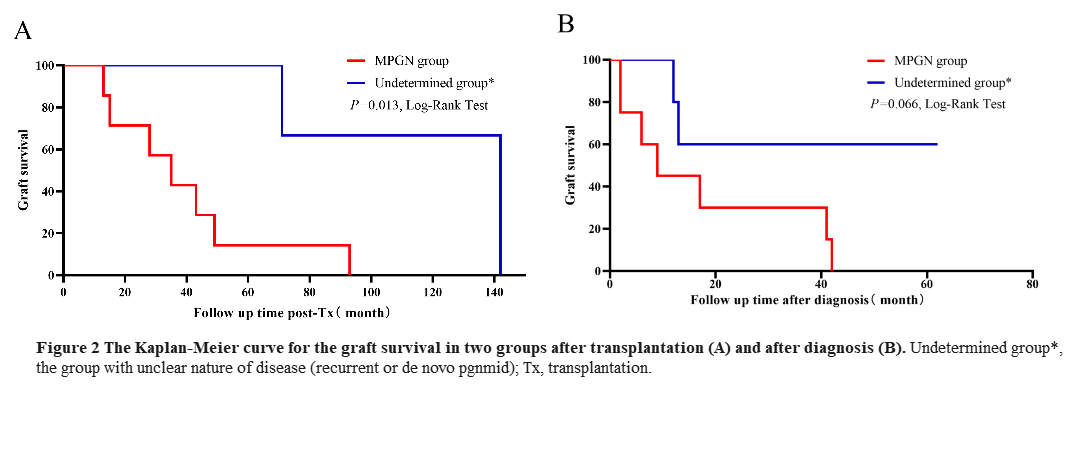
*Results: A total of 13 cases were enrolled. The median follow-up time was 43 months (range: 11-142 months) since kidney transplantation (KTx). Main clinical presentations at diagnosis included hematuria (92%) and proteinuria (100%). Median graft survival was 17 months from time of diagnostic biopsy, and was 49 months from Tx. Only 1 case showed IgGλ stripe through serum immunofixation electrophoresis. Light microscopy displayed MPGN (n=8), MN (n=2), MsGN (n=3). Immunofluorescence (IF) revealed IgG3κ (n=9), IgG3λ (n=2), IgG1κ (n=1) and IgG1λ (n=1). Except for the basic immunosuppressive therapies, partial cases received additional therapies including plasma exchange (n=3), pulse steroid (n=3), IVIG (n=2), bortezomib (n=7), rituximab (n=4). During the follow-up, nine cases progressed to dialysis, of which two cases died of infection. One case had complete response and one case had partial response after intensive therapies. Native kidney biopsy manifesting as MPGN was related to rapid diagnosis and poor prognosis compared to unknow primary glomerular diseaese.
*Conclusions: PGNMID in renal allografts represented mostly MPGN in LM and IgG3κ in IF in Chinese recepients, which progress rapidly once diagnosis. Recepients with primay MPGN should receive surveillance biopsy after KTx.
To cite this abstract in AMA style:
Wu Q, Liang D, Ni X, Song T, Wu X, Zhang M, Chen J, Cheng D, Jiqiu W. Poor Prognosis of Proliferative Glomerulonephritis with Monoclonal IgG Deposits in Renal Allografts: A Retrospective Multicenter Study from China [abstract]. Am J Transplant. 2022; 22 (suppl 3). https://atcmeetingabstracts.com/abstract/poor-prognosis-of-proliferative-glomerulonephritis-with-monoclonal-igg-deposits-in-renal-allografts-a-retrospective-multicenter-study-from-china/. Accessed March 30, 2026.« Back to 2022 American Transplant Congress