Donor-Derived Duodenal Adenocarcinoma of a Bladder-Drained Pancreas Allograft
1Northwestern University, Chicago, IL, 2Urology of St. Louis, St. Louis, MO, 3Mayo Clinic, Phoenix, AZ
Meeting: 2022 American Transplant Congress
Abstract number: 1506
Keywords: Malignancy, Pancreas, Pancreas transplantation, Urinalysis
Topic: Clinical Science » Organ Inclusive » 67 - Non-PTLD/Malignancies
Session Information
Session Time: 7:00pm-8:00pm
 Presentation Time: 7:00pm-8:00pm
Presentation Time: 7:00pm-8:00pm
Location: Hynes Halls C & D
*Purpose: Donor-derived malignancies are rare but frequently present with aggressive pathology and high mortality rates [PMID 32627325]. The urologic literature demonstrates an increased risk of adenocarcinomas of bowel segments used in bladder reconstruction, with most presenting 20-30 years after surgery [PMID 29169454]. This time frame presently corresponds to the 1990s, the peak era of pancreas transplants with exocrine drainage via anastomosis of allograft duodenum to recipient bladder. The bowel/bladder interface in bladder-drained pancreata is a potentially underappreciated site for neoplasia in patients with an already elevated cancer risk due to chronic immunosuppression.
*Methods: We present the case of a 57-year-old recipient of a failed bladder-drained simultaneous pancreas/kidney transplant who developed an adenocarcinoma of the duodenum of his allograft pancreas twenty-four years after transplantation.
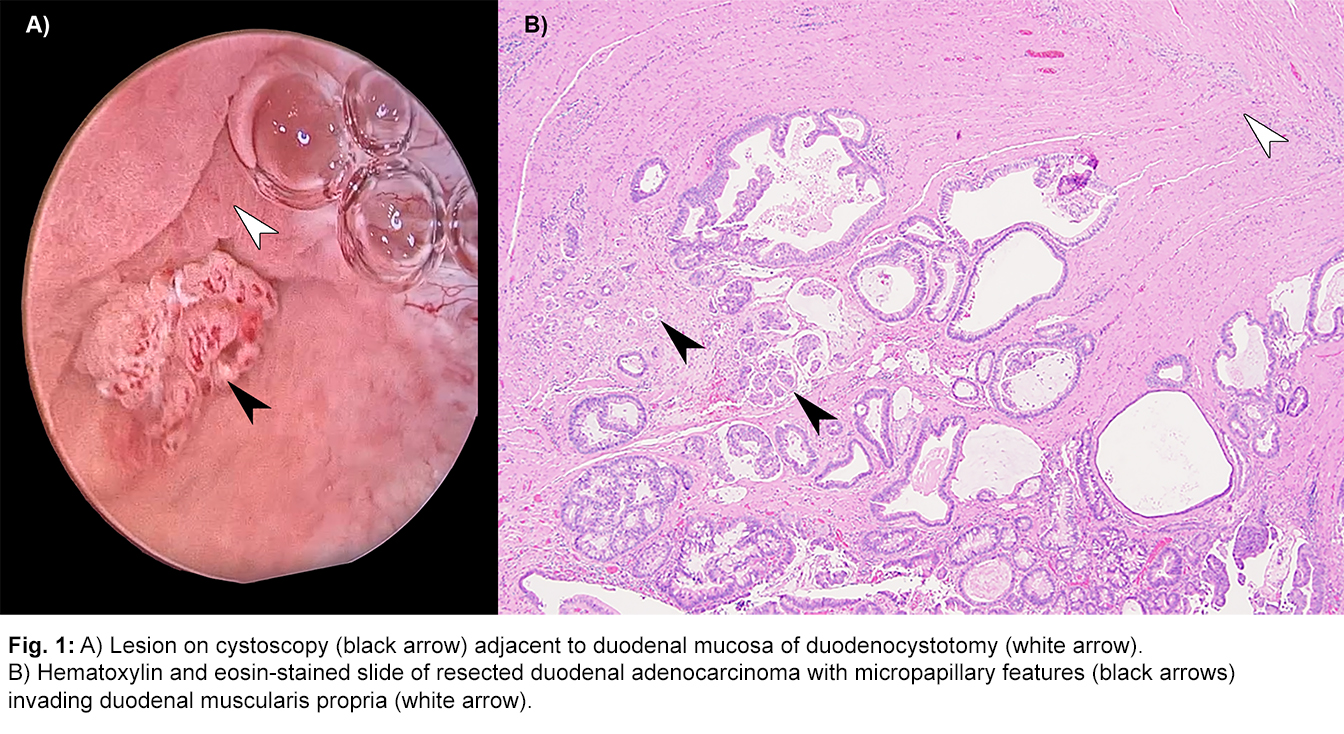
*Results: The patient was initially referred for evaluation of asymptomatic microhematuria with up to 51-100 RBC/HPF on multiple urinalyses. Cystoscopy revealed a lesion at the duodenocystotomy (Fig. 1A). Biopsies demonstrated the lesion was a tubular adenoma with high-grade dysplasia. The patient was counseled on the risk of an occult duodenal malignancy and elected for resection of his allograft pancreas/duodenum with a margin of adjacent bladder. This was accomplished via an intraperitoneal approach through a midline incision. Final pathology revealed a 1.0 cm adenocarcinoma with micropapillary features invading the muscularis propria of the duodenum, stage pT2 (Fig. 1B). All surgical margins, the donor pancreas and the resected portion of bladder were negative for carcinoma. He was treated with adjuvant capecitabine/oxaliplatin which was discontinued due to severe nausea. Surveillance cystoscopy and cross-sectional imaging have shown no evidence of recurrence nine months later.
*Conclusions: To the extent of our knowledge, this is the first description of a donor-derived duodenal adenocarcinoma of a bladder-drained pancreas allograft. This cancer presented twenty-four years after transplantation, a time frame comparable to that seen in malignancies of bowel segments used in bladder reconstruction. As the segment of the population with bladder-drained pancreata ages, malignancies of the donor duodenum and pancreas should be considered in recipients presenting with gross or microscopic hematuria.
To cite this abstract in AMA style:
Isaacson D, Steggerda J, Xue Y, Auffenberg GB, Katariya NN. Donor-Derived Duodenal Adenocarcinoma of a Bladder-Drained Pancreas Allograft [abstract]. Am J Transplant. 2022; 22 (suppl 3). https://atcmeetingabstracts.com/abstract/donor-derived-duodenal-adenocarcinoma-of-a-bladder-drained-pancreas-allograft/. Accessed June 1, 2026.« Back to 2022 American Transplant Congress