De Novo DSA Would Not Necessarily Cause Graft Rejection After Renal Transplantation: Characteristics of DSA Developing Biopsy-Proven Chronic Antibody-Mediated Rejection
Kidney Center, Nagoya Daini Red Cross Hospital, Nagoya, Japan.
Meeting: 2015 American Transplant Congress
Abstract number: 92
Keywords: Biopsy, HLA antibodies, Kidney transplantation
Session Information
Session Name: Concurrent Session: Kidney Antibody Mediated Rejection II
Session Type: Concurrent Session
Date: Sunday, May 3, 2015
Session Time: 4:00pm-5:30pm
 Presentation Time: 4:24pm-4:36pm
Presentation Time: 4:24pm-4:36pm
Location: Terrace I-III
Introduction:
De novo donor-specific HLA antibodies (dn DSA) production after renal transplantation has been reported to be associated with chronic antibody mediated rejection (CAMR), which leads to poor outcome. However, it is unclear whether all DSA can cause CAMR and what specificity of HLA antibodies is responsible for CAMR have been raised. The aim of our study was to examine (i) graft condition by indication biopsy in recipients with dn DSA and (ii) risk factors of developing subclinical CAMR.
Methods:
We studied 899 follow-up renal transplant recipients without pretransplant DSA. These patients were annually screened for HLA antibodies by LABScreen Mixed and DSA was identified by LABScreen single antigen beads. Among 96 DSA-positive patients (10.7%), renal graft biopsies were performed on 44 patients with dnDSA (MFI>1000) and without renal dysfunction. C1q binding testing was conducted in 44 patients using C1q screening kit.
Results:
Subclinical CAMR was diagnosed in 18 patients (40.9%) among 44 patients. Compared with no CAMR, subclinical CAMR group demonstrated younger recipients, higher DSA-MFI, increased MFI, positive C1q, past history of acute rejection, non-adherence and HLA-DR associated DSA. Among 26 patients with no CAMR, eight patients (30.8%) were proven to have no CAMR by re-biopsy after two years. The remaining 26 patients without CAMR diagnosis did not show renal dysfunction clinically, while 5 of 18 with CAMR deteriorated renal function even after rejection treatment such as double filtration plasmapheresis, rituximab and steroid pulse.
Conclusion:
All patients with dn DSA would not always cause CAMR. Therefore, graft biopsy might be essential for initiating rejection therapy based on definite diagnosis of CAMR. Characteristics of CAMR (Class II DSA; DR+DQ or DR, higher DSA MFI, increased DSA-MFI, past history of acute rejection, younger recipients, non-adherence and positive C1q) might be considered to be risk factors of developing subclinical CAMR in patients with dn DSA.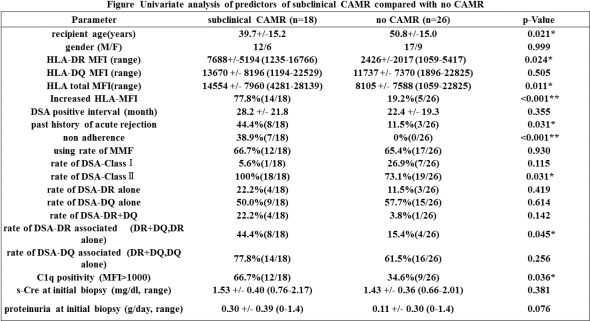 .
.
To cite this abstract in AMA style:
Yamamoto T, Watarai Y, Takeda A, Okada M, Tsujita M, Takahisa H, Goto N, Narumi S, Kobayashi T. De Novo DSA Would Not Necessarily Cause Graft Rejection After Renal Transplantation: Characteristics of DSA Developing Biopsy-Proven Chronic Antibody-Mediated Rejection [abstract]. Am J Transplant. 2015; 15 (suppl 3). https://atcmeetingabstracts.com/abstract/de-novo-dsa-would-not-necessarily-cause-graft-rejection-after-renal-transplantation-characteristics-of-dsa-developing-biopsy-proven-chronic-antibody-mediated-rejection/. Accessed May 29, 2026.« Back to 2015 American Transplant Congress