Clinical Significance of Estimated DSA MFI Values at 1,000 C1q MFI for Differentiation Between Harmful and Harmless DSA
1Aichi Medical University, Nagkute, Japan
2Nagoya Daini Red Cross Hospital, Nagoya, Japan
3Masuko Memorial Hospital, Nagoya, Japan
4Nagoya University School of Medicine, Nagoya, Japan.
Meeting: 2015 American Transplant Congress
Abstract number: B240
Keywords: HLA antibodies, Kidney transplantation, Rejection
Session Information
Session Name: Poster Session B: Translational Genetics and Proteomics in Transplantation
Session Type: Poster Session
Date: Sunday, May 3, 2015
Session Time: 5:30pm-6:30pm
 Presentation Time: 5:30pm-6:30pm
Presentation Time: 5:30pm-6:30pm
Location: Exhibit Hall E
INTRODUCTION
Control of chronic antibody mediated rejection (CAMR) is essential for further improvement of long-term graft survival. Early detection of de novo donor specific antibodies (DSA) is important, but the problem is that DSA would not necessarily cause CAMR. Recently, C1q binding assay has been developed, but its clinical significance remains controversial. We report the potential value of newly proposed analysis for assessing complement binding ability of DSA.
METHODS
31 follow up renal transplant recipients with de novo DSA were divided into two groups; CAMR (biopsy proven, n=19, DR: 3, DR+DQ: 5, DQ: 9, Class I: 2) and Stable (no CAMR, n=12, DQ: 12). The values of DSA and C1q were measured using LABScreen Single Antigen and C1q Screen kit. Scatter graph was obtained by plotting DSA MFI values on the horizontal (x) axis and C1q MFI on the vertical (y) axis. Estimated DSA MFI (e-DSA) values at 1000 C1q MFI were determined by least square regression line. 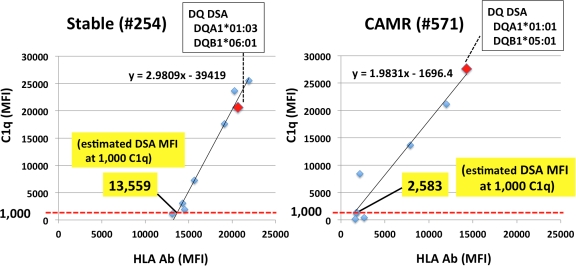 Low value means high complement binding capacity even at low antibody levels.
Low value means high complement binding capacity even at low antibody levels.
RESULTS
There are no significant differences in DSA (13500+/-6000 vs 15500+/-6500), C1q (15700+/-12700 vs 14600+/-10500), C1q positive rate (cutoff = 1000) (12/19; 63% vs 9/12; 75%) or e-DSA values at 1000 C1q (7800+/-3900 vs 11100+/-3400) between CAMR and Stable groups. However, CAMR was observed in 6/6 (100%) when e-DSA at 1000 C1q was below 6000, whereas CAMR was only in 7/17 (41%) when it was over 6000.
| CAMR (+) | CAMR (-) | |
| e-DSA at 1000 C1q ≥ 6000 | 7 | 10 |
| e-DSA at 1000 C1q < 6000 | 6 | 0 |
CONCLUSIONS
Analysis of e-DSA values at 1000 C1q can potentially distinguish between harmful and harmless DSA. There is a high possibility that DSA with high complement binding ability will cause CAMR, although DSA with low ability would not indicate no CAMR. HLA expression levels on graft endothelial cells also need to be considered.
To cite this abstract in AMA style:
Horimi K, Akaza T, Kuroki K, Sakamoto S, Matsuoka Y, Watarai Y, Narumi S, Katayama A, Uchida K, Kobayashi T. Clinical Significance of Estimated DSA MFI Values at 1,000 C1q MFI for Differentiation Between Harmful and Harmless DSA [abstract]. Am J Transplant. 2015; 15 (suppl 3). https://atcmeetingabstracts.com/abstract/clinical-significance-of-estimated-dsa-mfi-values-at-1000-c1q-mfi-for-differentiation-between-harmful-and-harmless-dsa/. Accessed May 27, 2026.« Back to 2015 American Transplant Congress