Center and Surgeons' Experience Improves Outcome in Adult-to-Adult Living Donor Liver Transplantation: Validation of the Report of the A2ALL Consortium.
Transplant and Hepatobiliary Surgery, Henry Ford Hospital, Detroit, MI.
Meeting: 2016 American Transplant Congress
Abstract number: A221
Keywords: Bile duct, Graft survival, Living-related liver donors, Risk factors
Session Information
Session Name: Poster Session A: Living Donor Liver Transplantation
Session Type: Poster Session
Date: Saturday, June 11, 2016
Session Time: 5:30pm-7:30pm
 Presentation Time: 5:30pm-7:30pm
Presentation Time: 5:30pm-7:30pm
Location: Halls C&D
Background: Adult-to-adult living donor liver transplantation cohort study (A2ALL) has reported improved outcomes in centers with greater experience (>20 cases). The aim of this study was to validate and investigate the influence of center's and surgeons' experience by reviewing living donor liver transplantation (LDLT) outcomes in non-A2ALL single center.
Methods: LDLT from December 2000 to March 2015 was reviewed (n=90). Risk factor analysis for graft survival and postoperative biliary complications (leak [BL] and anastomotic stricture [BAS]) were conducted. Surgeons' and center's experience were included in potential factors. Surgeons A, B and C performed 75 (between center's case #1-89, 2000-2015), 8 (between case#15-25, 2005-2006), and 7 LDLTs (between case #73-90, 2011-2015), respectively.
Results: Graft survival in the center's first 20 cases was significantly worse (P=0.01, hazard ratio [HR]=3.57). Surgeon A's first 20 cases (early experience) was considered to be a risk factor of worse graft survival (P=0.01, HR=4.02 [Ref. Surgeon A's late experience]), but not surgeons B's and C's early experience (P=0.16 and 0.99, respectively). 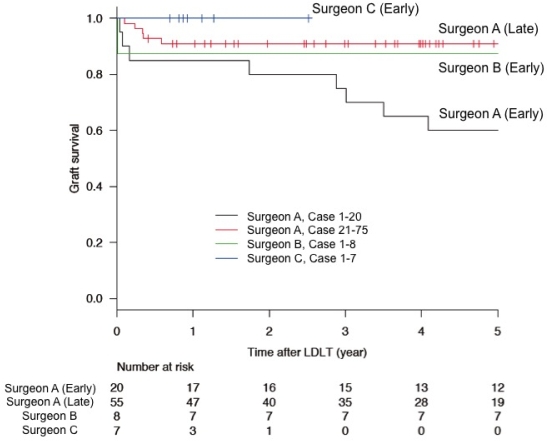 BL and BAS rates were 24% (22/90) and 19% (17/90). Surgeons A's and C's early experience remained independent risk factors for BL (P=0.01 and 0.02, odds ratio [OR]=3.96 and 7.67, respectively), along with recipient age (P=0.01, OR=1.06 per year) on multivariate analysis. Surgeon B's early experience increased a risk of BL, but not significant (P=0.27, OR=2.88). Type of biliary reconstruction (duct-to-duct vs. Roux-en-Y) or the number of ducts reconstructed was not a risk factor for BL. Center's or each surgeon's experience was not associated with BAS and no significant risk factors were identified.
BL and BAS rates were 24% (22/90) and 19% (17/90). Surgeons A's and C's early experience remained independent risk factors for BL (P=0.01 and 0.02, odds ratio [OR]=3.96 and 7.67, respectively), along with recipient age (P=0.01, OR=1.06 per year) on multivariate analysis. Surgeon B's early experience increased a risk of BL, but not significant (P=0.27, OR=2.88). Type of biliary reconstruction (duct-to-duct vs. Roux-en-Y) or the number of ducts reconstructed was not a risk factor for BL. Center's or each surgeon's experience was not associated with BAS and no significant risk factors were identified.
Conclusion: Once center experience reached 20 LDLTs, early experience of new surgeons no longer affected graft survival. However, regardless of center's experience, BL was consistently associated with surgeons' early experience. Surgeon's technical experience may play an important role in complex biliary reconstructions.
CITATION INFORMATION: Nagai S, Yoshida A, Rizzari M, Collins K, Kim D, Abouljoud M. Center and Surgeons' Experience Improves Outcome in Adult-to-Adult Living Donor Liver Transplantation: Validation of the Report of the A2ALL Consortium. Am J Transplant. 2016;16 (suppl 3).
To cite this abstract in AMA style:
Nagai S, Yoshida A, Rizzari M, Collins K, Kim D, Abouljoud M. Center and Surgeons' Experience Improves Outcome in Adult-to-Adult Living Donor Liver Transplantation: Validation of the Report of the A2ALL Consortium. [abstract]. Am J Transplant. 2016; 16 (suppl 3). https://atcmeetingabstracts.com/abstract/center-and-surgeons-experience-improves-outcome-in-adult-to-adult-living-donor-liver-transplantation-validation-of-the-report-of-the-a2all-consortium/. Accessed June 2, 2026.« Back to 2016 American Transplant Congress