Late Outcome Surrogate Score (LOSS) for Kidney Allograft Failure.
Comprehensive Transplant Center, Northwestern University, Chicago, IL.
Meeting: 2016 American Transplant Congress
Abstract number: A232
Keywords: Biopsy, Graft function, Graft survival, Kidney transplantation
Session Information
Session Name: Poster Session A: Long Term Outcomes in Kidney Transplantation
Session Type: Poster Session
Date: Saturday, June 11, 2016
Session Time: 5:30pm-7:30pm
 Presentation Time: 5:30pm-7:30pm
Presentation Time: 5:30pm-7:30pm
Location: Halls C&D
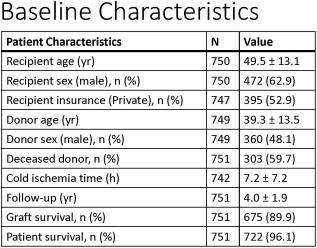
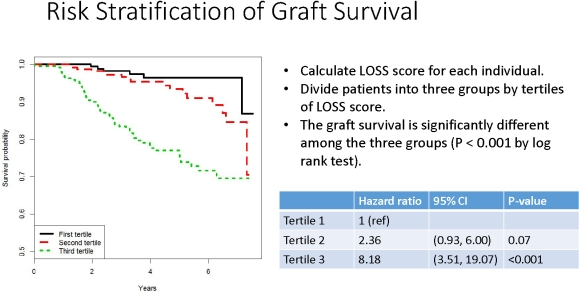
Background. Early outcomes following kidney transplant have steadily improved. Longer-term outcomes, while not the focus of regulatory oversight, are of vital importance. Clinical trials are difficult to power toward early survival metrics such that cost and sample size undermine feasibility. Current predictive models are sub-optimal. We developed a Late Outcome Surrogate Score (LOSS). Methods. We performed a retrospective, single-center study of kidney recipients (n=751) performed between January 2008 and December 2014 who underwent a 1-year protocol biopsy. Biopsies were scored by a single pathologist using Banff 2007 criteria. Graft survival was analyzed by Kaplan-Meier and log-rank methods. Demographic, serum creatinine, urine protein, anti-HLA donor specific antibodies (DSA) and biopsy data were extracted from Northwestern University (NU ORBIT) database. Stepwise variable selection was used to build a multivariate Cox proportional hazards model to predict 6-year graft survival. Covariates were assessed for discrimination using C-statistics. Integrated discrimination improvement (IDI) and net reclassification index (NRI) were used to determine the incremental value of covariates in risk prediction. Results. Baseline characteristics are depicted (Table). Serum creatinine, urine protein, antibody mediated rejection and interstitial inflammation were associated with graft loss (Table). The C-statistic was 0.77 (95% CI 0.72, 0.83. Biopsy results significantly improved IDI and NRI by 0.04 (95% CI 0.00, 0.10) and 0.24 (95% CI 0.10, 0.37), respectively. Increasing tertiles of LOSS demonstrated a marked decline in graft survival (p < 0.001 by log rank; Figure). Conclusion. LOSS is a good predictor of longer-term kidney allograft survival. Further model refinement might lead to development of a suitable proxy for use in clinical trials.
CITATION INFORMATION: Ho B, Zhao L, Montag S, Ladner D, Abecassis M, Skaro A. Late Outcome Surrogate Score (LOSS) for Kidney Allograft Failure. Am J Transplant. 2016;16 (suppl 3).
To cite this abstract in AMA style:
Ho B, Zhao L, Montag S, Ladner D, Abecassis M, Skaro A. Late Outcome Surrogate Score (LOSS) for Kidney Allograft Failure. [abstract]. Am J Transplant. 2016; 16 (suppl 3). https://atcmeetingabstracts.com/abstract/late-outcome-surrogate-score-loss-for-kidney-allograft-failure/. Accessed April 30, 2026.« Back to 2016 American Transplant Congress