Perioperative Anidulafungin Combined with Triazole Prophylaxis for the Prevention of Early Invasive Candidiasis in Lung Transplant Recipients
1University of Colorado Skaggs School of Pharmacy, Aurora, CO, 2Division of Pulmonary Sciences and Critical Care, University of Colorado, Denver, CO, 3Division of Infectious Disease, University of Colorado, Denver, CO, 4Baylor University Medical Center, Dallas, TX
Meeting: 2021 American Transplant Congress
Abstract number: 765
Keywords: Fungal infection, Lung transplantation, Prophylaxis, Survival
Topic: Clinical Science » Infectious Disease » All Infections (Excluding Kidney & Viral Hepatitis)
Session Information
Session Name: All Infections (Excluding Kidney & Viral Hepatitis)
Session Type: Poster Abstract
Session Date & Time: None. Available on demand.
Location: Virtual
*Purpose: Invasive candidiasis (IC) is a substantial cause of morbidity and mortality in lung transplant recipients (LTRs). Post-operative factors, such as prolonged hospital stay, central lines, delayed chest closure, and dehiscence increase early IC risk. Guidelines propose targeted IC coverage in the first 2-4 weeks with fluconazole or an echinocandin. To our knowledge, this is the first study investigating combination triazole/echinocandin use in the early post-LT period.
*Methods: We retrospectively assessed a recent protocol at our center. LTRs from 1/2016 to 1/2020 receiving in-hospital anidulafungin and triazole prophylaxis (protocol) were compared to LTRs receiving triazole prophylaxis alone (pre-protocol). Itraconazole was the preferred triazole and was started once tolerating oral medications and continued for at least one year in both cohorts. The primary outcome was IC at 90 days.
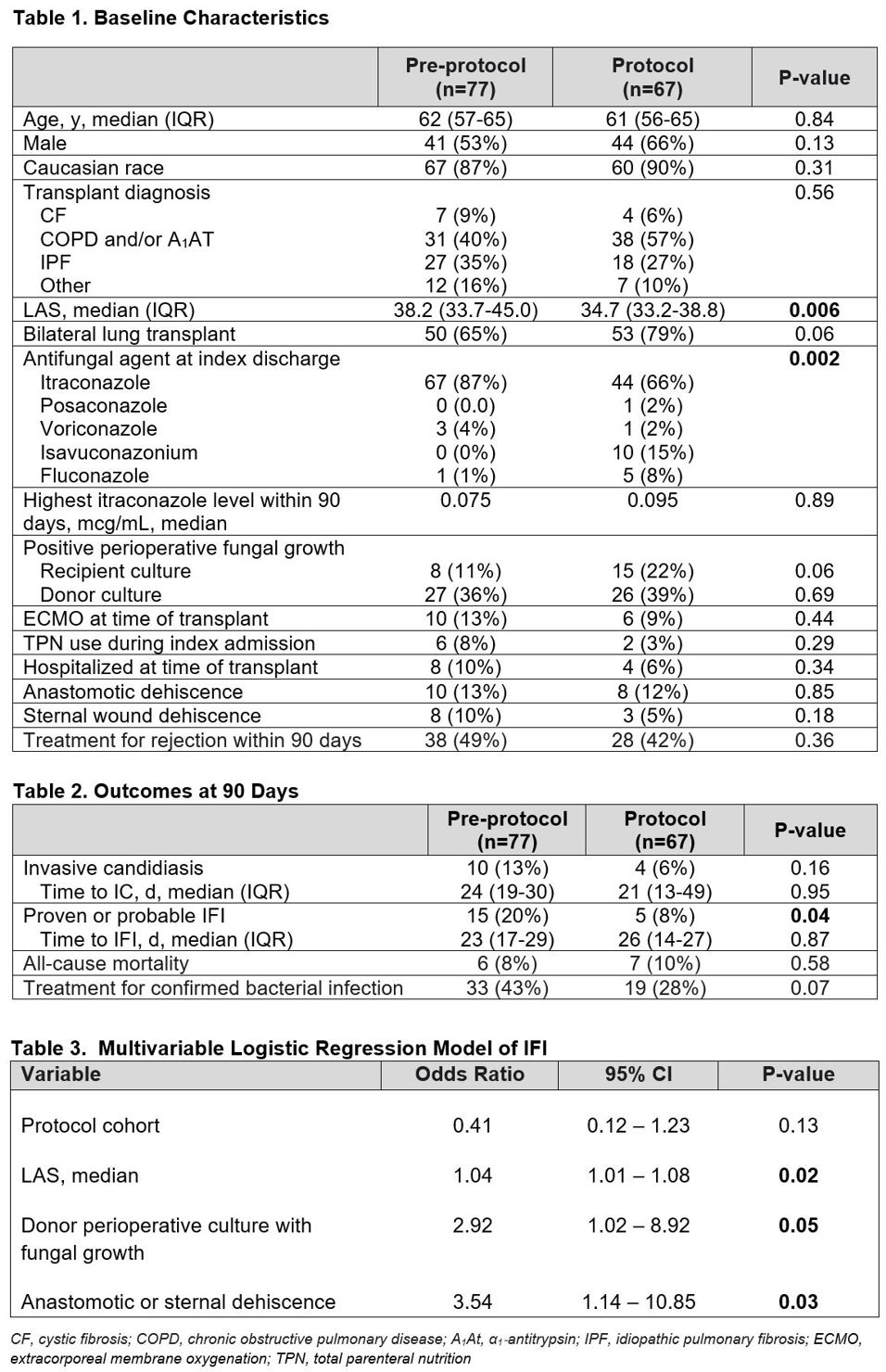
*Results: A total of 144 LTRs were analyzed. Baseline characteristics were similar, except lower lung allocation score (LAS) and more alternative triazole antifungal use in the protocol group (Table 1). Median duration of anidulafungin was 12 days. There was a numerically lower incidence of IC in the protocol group, although not statistically significant (6% vs 13%, Table 2). Incidence of IFI was lower in the protocol group. However, when controlling for LAS, donor fungal colonization, and dehiscence in multivariable analysis, protocol cohort was not significantly associated with IFI. Triazole antifungal type was not included in this model as a univariate analysis did not reveal a meaningful association with IFI. There was no difference in bacterial infections or all-cause mortality.
*Conclusions: In-hospital anidulafungin for early IC prevention offers unclear benefit when used in combination with triazole prophylaxis among LTRs. LAS, donor fungal colonization, and dehiscence were significantly associated with overall IFI; however, protocol cohort assignment was not. Overall, the findings of this single-center study do not support the use of universal triazole/echinocandin prophylaxis in LTRs. Further studies of alternate strategies for early IC prevention in lung transplant recipients are warranted.
To cite this abstract in AMA style:
Sartain E, Schoeppler K, Crowther B, Smith JB, Abidi M, Grazia TJ, Steele M, Gleason T, Porter K, Gray A. Perioperative Anidulafungin Combined with Triazole Prophylaxis for the Prevention of Early Invasive Candidiasis in Lung Transplant Recipients [abstract]. Am J Transplant. 2021; 21 (suppl 3). https://atcmeetingabstracts.com/abstract/perioperative-anidulafungin-combined-with-triazole-prophylaxis-for-the-prevention-of-early-invasive-candidiasis-in-lung-transplant-recipients/. Accessed May 19, 2026.« Back to 2021 American Transplant Congress