MELD-Na Score Based Liver Allocation: Hyponatremia is No Longer a Risk Factor for Waitlist Mortality
1Transplant and Hepatobiliary Surgery, Henry Ford Hospital, Detroit, MI
2Gastroenterology, Henry Ford Hospital, Detroit, MI.
Meeting: 2018 American Transplant Congress
Abstract number: A264
Keywords: Liver cirrhosis, Liver transplantation, Multivariate analysis, Waiting lists
Session Information
Session Name: Poster Session A: Liver: MELD, Allocation and Donor Issues (DCD/ECD)
Session Type: Poster Session
Date: Saturday, June 2, 2018
Session Time: 5:30pm-7:30pm
 Presentation Time: 5:30pm-7:30pm
Presentation Time: 5:30pm-7:30pm
Location: Hall 4EF
Background: Hyponatremia is associated with an increased risk of liver transplant (LT) waitlist mortality. The aim of this study was to compare waitlist outcomes between the MELD and MELD-Na based liver allocation.
Methods: We examined two patient groups from the UNOS registry; MELD-era group composed of patients who were registered between July 1, 2013 and December 31, 2015 (n=18,014) and MELD-Na era group composed of patients who were registered between Jan. 1, 2016 and Mar. 31, 2017 (n=10,187). Waitlist outcomes and association with serum sodium concentration were evaluated in these two eras using Cox multivariable analysis.
Results: The hazard of waitlist mortality among those in the MELD-Na era is 37.9% lower than the hazard among the MELD era, after adjusting for other covariates in the model (Hazard ratio [HR]=0.621, P<0.001). The hazard of waitlist mortality in patients with mild, moderate and severe hyponatremia (130-134, 125-129, <125mmol/L) is 1.323, 1.571 and 2.337 times the hazard in comparison to those with normal sodium level (135-145mmol/L) (P <0.001, <0.001 and <0.001, respectively), but this adverse impact decreased by 24.9% (1.323-0.993/1.323), 26.9% (1.571-1.148/1.571), and 39.1% (2.337-1.421/2.337) in the MELD-Na era (HR =0.993, 1.148 and 1.421, P =0.94, 0.256 and 0.041 in those with mild, moderate and severe hyponatremia, respectively). The risk associated with hyponatremia was more prominent in patients with low-mid scores (6-26) in the MELD era, which was no longer observed in the MELD-Na era.
The hazard of waitlist mortality in patients with mild, moderate and severe hyponatremia (130-134, 125-129, <125mmol/L) is 1.323, 1.571 and 2.337 times the hazard in comparison to those with normal sodium level (135-145mmol/L) (P <0.001, <0.001 and <0.001, respectively), but this adverse impact decreased by 24.9% (1.323-0.993/1.323), 26.9% (1.571-1.148/1.571), and 39.1% (2.337-1.421/2.337) in the MELD-Na era (HR =0.993, 1.148 and 1.421, P =0.94, 0.256 and 0.041 in those with mild, moderate and severe hyponatremia, respectively). The risk associated with hyponatremia was more prominent in patients with low-mid scores (6-26) in the MELD era, which was no longer observed in the MELD-Na era.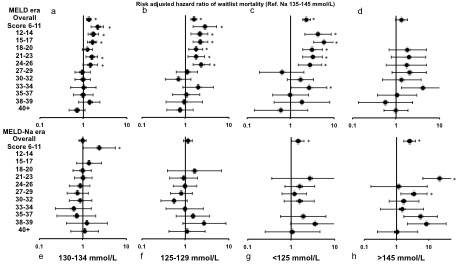
Conclusions: The new liver allocation system based on MELD-Na score successfully decreased the risk of waitlist mortality in patients with hyponatremia.
CITATION INFORMATION: Nagai S., Chau L., Safwan M., Schilke R., Rizzari M., Collins K., Yoshida A., Abouljoud M., Moonka D. MELD-Na Score Based Liver Allocation: Hyponatremia is No Longer a Risk Factor for Waitlist Mortality Am J Transplant. 2017;17 (suppl 3).
To cite this abstract in AMA style:
Nagai S, Chau L, Safwan M, Schilke R, Rizzari M, Collins K, Yoshida A, Abouljoud M, Moonka D. MELD-Na Score Based Liver Allocation: Hyponatremia is No Longer a Risk Factor for Waitlist Mortality [abstract]. https://atcmeetingabstracts.com/abstract/meld-na-score-based-liver-allocation-hyponatremia-is-no-longer-a-risk-factor-for-waitlist-mortality/. Accessed May 28, 2026.« Back to 2018 American Transplant Congress