Measuring and Monitoring Equity in Access to Deceased Donor Lung Transplants among Lung Registrations
1Research, United Network for Organ Sharing, Richmond, VA, 2University of Washington, Seattle, WA, 3St. Louis Children's Hospital, St. Louis, MO
Meeting: 2020 American Transplant Congress
Abstract number: 394
Keywords: Lung, Lung transplantation, Monitoring, Outcome
Session Information
Session Name: Lung: Let's Start at the Beginning: Pre-Transplant Decision Making and Access to Lung Donors
Session Type: Oral Abstract Session
Date: Saturday, May 30, 2020
Session Time: 3:15pm-4:45pm
 Presentation Time: 4:03pm-4:15pm
Presentation Time: 4:03pm-4:15pm
Location: Virtual
*Purpose: In 2018, the Organ Procurement and Transplantation Network (OPTN) published a methodology to measure equity in access to deceased donor kidney transplantation that has since been applied to lung allocation. The analytical approach is designed to measure disparities related to geographic, demographic, clinical, and socioeconomic factors while adjusting for factors used to prioritize candidates for allocation, as well as to quantify system-level equity as a single number that can be tracked over time.
*Methods: OPTN data on active lung candidates were used to fit 36 separate Poisson transplant rate models, adjusting for 15 candidates covariates, over rolling 6-month periods examined quarterly from 1/2010 to 6/2019. Disparity was quantified as the Winsorized standard deviation (SDw) of the predicted transplant rates (on log scale) among lung registrations, after “discounting” for desired, policy-induced disparities such as the lung allocation score by holding these factors constant. Risk-adjusted, factor-specific disparities were calculated as the SDw of the log(transplant rate), holding all other factors constant.
*Results: Despite 3 policy modifications over the time period, including the removal of donation service area (DSA), the overall disparity metric has remained very stable (fig1). DSA was the factor most independently associated with disparities in access to transplant in each period. Other factors that rose to the top, but well below DSA, include gender, ethnicity, diagnosis group, and age.
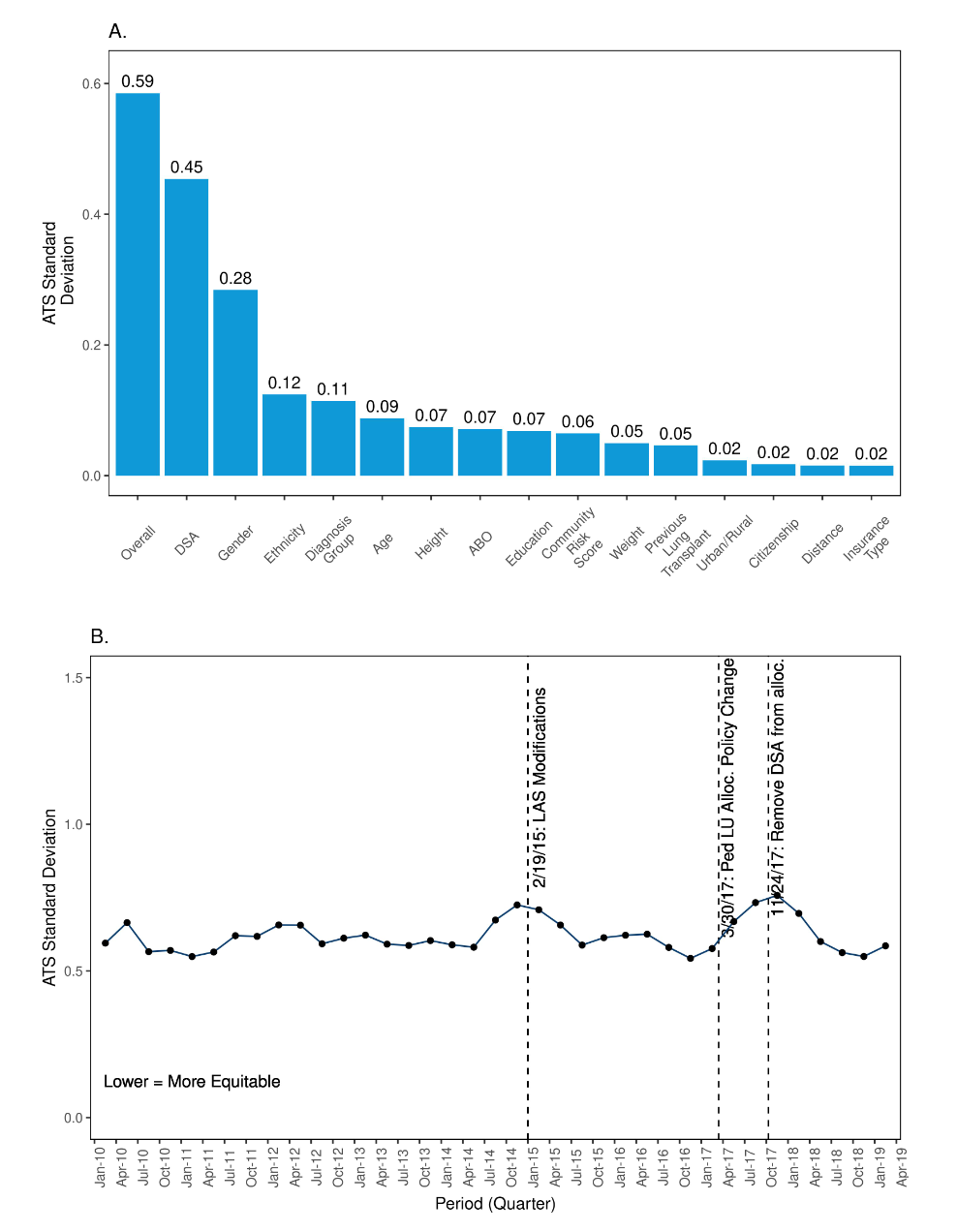
*Conclusions: Even after removing DSA as a unit of allocation for lung in 2017, DSA is the factor contributing the most to inequities. This methodology will be used for monitoring the impact on equity of future policy changes, such as the anticipated transition to “Continuous Distribution” for lungs.
To cite this abstract in AMA style:
Goff RR, Lease ED, Sweet S, Robinson A, Stewart D. Measuring and Monitoring Equity in Access to Deceased Donor Lung Transplants among Lung Registrations [abstract]. Am J Transplant. 2020; 20 (suppl 3). https://atcmeetingabstracts.com/abstract/measuring-and-monitoring-equity-in-access-to-deceased-donor-lung-transplants-among-lung-registrations/. Accessed May 28, 2026.« Back to 2020 American Transplant Congress