Measuring and Monitoring Equity in Access to Deceased Donor Liver Transplants
UNOS, Richmond.
Meeting: 2018 American Transplant Congress
Abstract number: A261
Keywords: Allocation, Liver transplantation, Waiting lists
Session Information
Session Name: Poster Session A: Liver: MELD, Allocation and Donor Issues (DCD/ECD)
Session Type: Poster Session
Date: Saturday, June 2, 2018
Session Time: 5:30pm-7:30pm
 Presentation Time: 5:30pm-7:30pm
Presentation Time: 5:30pm-7:30pm
Location: Hall 4EF
Background: In 2016, the Organ Procurement and Transplantation Network (OPTN) developed a methodology to measure equity in deceased donor kidney allocation and has adapted it for liver. The approach departs from the use of median MELD at transplant (MMAT) to measure geographic disparity, since the goal was an aggregate disparity metric that captures transplant access differences in across a broad range of candidate factors (demographic, clinical, socioeconomic), not solely Donor Service Area (DSA) of listing.
Methods: We fit separate Cox models for 29 quarterly, period-prevalent cohorts of active liver candidates ever waiting from 1/2010 to 3/2017, adjusting for 16 candidate covariates. Medical urgency status and allocation MELD/PELD were time-dependent. We measured disparity using the Winsorized standard deviation (SDw) of the linear predictors (Access-to-Transplant Score, ATS) for all candidates waiting on 1/1/2017, after “discounting” for variability associated with urgency status and MELD/PELD – which induce intentional disparities – by holding these factors constant. Risk-adjusted, factor-specific disparities were measured as the SD of ATS, holding all other factors constant.
Results: Aggregate disparity remained relatively stable over the study period with SDw at around 0.80 (Fig 1). 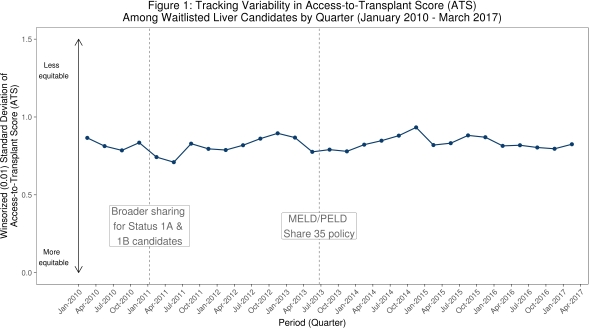
All else equal, DSA (SDw=0.72) was the factor most associated with disparity, followed by age and ABO (Fig 2). 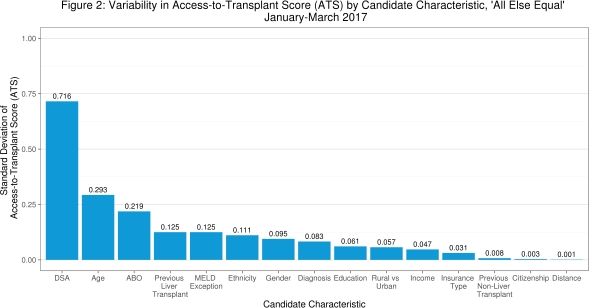
In 1Q2017, DSAs with higher average ATS tended to have lower MMAT: Pearson rho=-0.72, 95% CI: (-0.83, -0.55).
Conclusions: Despite previous liver policy changes, which were aimed primarily at reducing waiting list mortality, the aggregate measure of disparity did not change appreciably over the past 7 years. Even more so than for kidney, disparities in liver access by DSA far exceeded disparities associated with other factors. Transplant access by DSA was generally consistent as measured by ATS vs. MMAT.
CITATION INFORMATION: Stewart D., Robinson A., Harper A., Klassen D. Measuring and Monitoring Equity in Access to Deceased Donor Liver Transplants Am J Transplant. 2017;17 (suppl 3).
To cite this abstract in AMA style:
Stewart D, Robinson A, Harper A, Klassen D. Measuring and Monitoring Equity in Access to Deceased Donor Liver Transplants [abstract]. https://atcmeetingabstracts.com/abstract/measuring-and-monitoring-equity-in-access-to-deceased-donor-liver-transplants/. Accessed May 25, 2026.« Back to 2018 American Transplant Congress