Lessons Learned Transplanting High KDPI Kidneys Over a Decade: Improvements in Graft Survival Stem from Lower Rates of Early Graft Loss.
1Duke University Medical Center, Durham, NC
2CTI Clinical Trial and Consulting Services, Raleigh, NC.
Meeting: 2016 American Transplant Congress
Abstract number: 563
Keywords: Graft survival, Kidney transplantation, Outcome
Session Information
Session Name: Concurrent Session: The High KDPI Kidney: Outcomes and Optimal Utilization
Session Type: Concurrent Session
Date: Tuesday, June 14, 2016
Session Time: 4:30pm-6:00pm
 Presentation Time: 5:18pm-5:30pm
Presentation Time: 5:18pm-5:30pm
Location: Ballroom C
Purpose. The Kidney Donor Profile Index (KDPI) recently replaced SCD/ECD designations, to provide transplant centers a more precise estimate of predicted graft survival, with the highest risk organs labeled “KDPI>85%”. We examined historical trends in graft survival and risk of graft loss in a time-dependent fashion from the transplant event, among kidneys with KDPI>85% used over the past decade.
Methods. We examined adult recipients (≥18) of deceased donors Jan 2000 to Dec 2012, excluding multi-organ and repeat transplant recipients (N=92,935). Donor, recipient, and transplant characteristics were examined by era: 2000-2002 (era1; n=19,235), 2003-2006 (era2; n=27,778), 2007-2012 (era3; n=45,922). Graft survival was estimated using Kaplan-Meier method. Modified Bailey-Makeham parametric model for the hazard of graft failure (AJT 2009; 9(S2):641) was used to evaluate risk of graft loss from the transplant event.
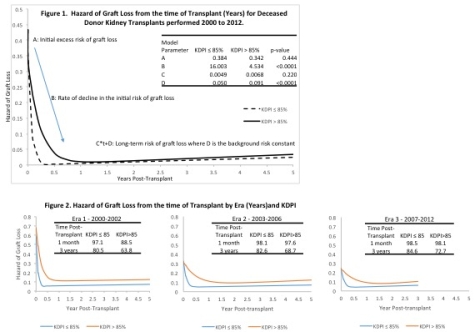
Results. In successive eras: 8.5%, 10%, and 10.9% of allografts had a KDPI>85%. Donors had increasing prevalence of DM, HTN, high BMI. More DCD organs were used. Recipients were older, more often African-American, more often had DM and high BMI. Three year graft survival increased in both KDPI groups. Hazard of graft loss from the time of transplant, by KDPI, is depicted for the entire cohort in Figure 1. Initial risk of graft loss was similar between KDPI groups, though early post-txp (<6 months) the rate of decline in risk is less pronounced among KDPI>85% organs. The long-term risk (>1-year) remained higher among KDPI>85% organs, likely from increased background risk. Across eras, there was a decrease in initial and background risks, most pronounced among KDPI>85% organs (Figure 2).
Conclusions. Graft survival for KDPI>85% organs increased 2000 to 2012, despite higher risk organs and recipients. The hazard of graft loss decreased significantly across eras; especially immediately post-transplant, suggesting that improvements in graft survival over the past decade may be attributable to less graft failure in the early post-operative period.
CITATION INFORMATION: Sanoff S, Ravindra K, Vikraman D, Patel U, Sudan D, Irish W. Lessons Learned Transplanting High KDPI Kidneys Over a Decade: Improvements in Graft Survival Stem from Lower Rates of Early Graft Loss. Am J Transplant. 2016;16 (suppl 3).
To cite this abstract in AMA style:
Sanoff S, Ravindra K, Vikraman D, Patel U, Sudan D, Irish W. Lessons Learned Transplanting High KDPI Kidneys Over a Decade: Improvements in Graft Survival Stem from Lower Rates of Early Graft Loss. [abstract]. Am J Transplant. 2016; 16 (suppl 3). https://atcmeetingabstracts.com/abstract/lessons-learned-transplanting-high-kdpi-kidneys-over-a-decade-improvements-in-graft-survival-stem-from-lower-rates-of-early-graft-loss/. Accessed May 25, 2026.« Back to 2016 American Transplant Congress