Influence of Converting Kidney Transplant Recipients with High Tacrolimus Variability to the Once Daily LCP Tac Formulation
Med Univ of South Carolina, Charleston, SC
Meeting: 2022 American Transplant Congress
Abstract number: 415
Keywords: FK506, Graft survival, Kidney, Rejection
Topic: Clinical Science » Kidney » 38 - Kidney Immunosuppression: Novel Regimens and Drug Minimization
Session Information
Session Name: Kidney Immunosuppression
Session Type: Rapid Fire Oral Abstract
Date: Tuesday, June 7, 2022
Session Time: 3:30pm-5:00pm
 Presentation Time: 4:30pm-4:40pm
Presentation Time: 4:30pm-4:40pm
Location: Hynes Room 302
*Purpose: Tacrolimus (Tac) is the cornerstone of immunosuppression used in kidney transplant recipients (KTRs). Tac high variability, low time in therapeutic range and non-adherence are significantly associated with poor long-term outcomes. The influence of converting to once daily, extended-release LCP-Tac on those with high variability in KTR is not well-studied.
*Methods: This was a single-center, retrospective cohort study of adult KTRs converted from Tac IR to LCP-Tac who were at least 1-yr post-transplant. Primary outcomes were to assess tac variability, using the coefficient of variation (CV), measured in trough levels drawn in the ambulatory setting from 3-12 months post-transplant, compared to steady-state levels drawn after conversion to LCP-Tac. High Tac variability was defined as Tac CV >30%. Time in therapeutic range (TITR) was also measured using the modified Rosendaal method. Univariate paired tests were utilized for statistical comparison and inferences.
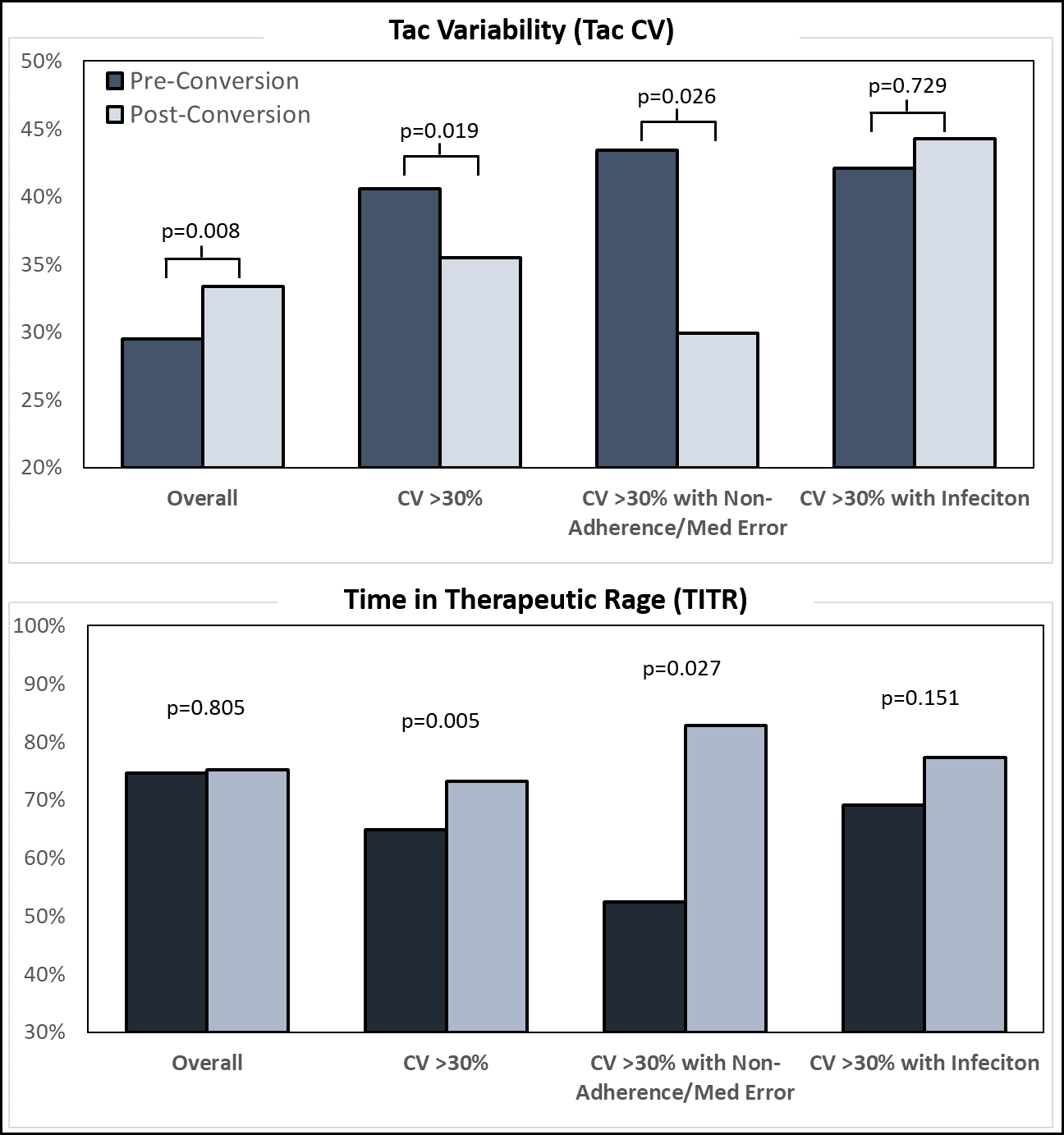
*Results: There were 193 KTRs included in this LCP-Tac conversion analysis, with a mean follow-up of 3.2±0.7 years and 1.3±0.3 years since conversion. The mean age was 52±13 years; 70% were African American, 39% were female, mean of 4 HLA mismatches, 44% cPRA, 16% living donor and 12% DCD. Tac CV was 29.5% before conversion, which increased to 33.4% after LCP-Tac (p=0.008). In those with Tac CV >30% (n=86), conversion to LCP-Tac reduced variability (40.6% vs. 35.5%; p=0.019) and for those with Tac CV >30% and non-adherence or med errors (n=16), LCP-Tac conversion substantially reduced Tac CV (43.4% vs 29.9%; p=0.026; Top Figure). TITR was similar before and after LCP-Tac conversion for the overall cohort (74.6% vs. 75.2%; p=0.805), while TITR significantly improved for those with high Tac CV with (52.4% vs. 82.8%; p=0.027) or without (64.8% vs. 73.2%; p=0.005; Bottom Figure) non-adherence or med errors. Infection with high Tac CV did not appreciably influence variability or TITR. In the overall cohort, 3% had rejection before conversion and 2% after (p=NS). At end of follow-up, graft and patient survival were 94% and 96%, respectively.
*Conclusions: In those with high Tac CV, conversion to LCP-Tac is associated with a significant reduction in variability and improvement in TITR, particularly in those with a history of documented non-adherence or those prone to medication errors.
To cite this abstract in AMA style:
Taber D, Bartlett F, Patel N, Sprague T, Patel S, Newman J, Andrade E, Rao N, Posadas A, Rao V, Casey M, Dubay D, Rohan V. Influence of Converting Kidney Transplant Recipients with High Tacrolimus Variability to the Once Daily LCP Tac Formulation [abstract]. Am J Transplant. 2022; 22 (suppl 3). https://atcmeetingabstracts.com/abstract/influence-of-converting-kidney-transplant-recipients-with-high-tacrolimus-variability-to-the-once-daily-lcp-tac-formulation/. Accessed May 17, 2026.« Back to 2022 American Transplant Congress