Induction Therapy (IT) in Simultaneous Pancreas and Kidney Transplantation (SPK) according to Patient Risk – A Registry Analysis
1Department of Surgery, University of Arizona, Tucson, AZ
2College of Public Health, University of Arizona, Tucson, AZ.
Meeting: 2015 American Transplant Congress
Abstract number: 227
Keywords: Induction therapy, Pancreas transplantation
Session Information
Session Name: Concurrent Session: Optimizing Immunosuppression in Pancreas Transplantation
Session Type: Concurrent Session
Date: Monday, May 4, 2015
Session Time: 2:15pm-3:45pm
 Presentation Time: 2:15pm-2:27pm
Presentation Time: 2:15pm-2:27pm
Location: Room 119-B
Purpose: Optimal IT in SPK recipients (rec) according to patient risk has not been studied.
Methods: Using the International Pancreas Transplant Registry database, we analyzed IT in 3,936 primary deceased-donor (DD) SPKs between 1/1/09 to 31/12/13. Patients (pt) who received depleting in combination with depleting AB were excluded.
We analyzed 2 homogenous pt groups: group 1 (n=1,694) was defined as low-risk (0% PRA, White, Age >35 years, BMI < 30 kg/m2) and group 2 (n=295) as high-risk (>10%PRA, Non-Whites, Age <35years of age). Five types of IT were compared: (1) depleting (TMG,ATG), >= 4d; (2) depleting (TMG,ATG), < 4d; (3) depleting (Campath), 1d; (4) non-depleting, 1-2d; (5) no IT. Only pts on maintenance therapy with tacrolimus and MMF were included.
Results: In group 1 (low-risk), the different types of IT did not result in any significant differences in pt (p=0.40) or graft survival rates (p>0.82): at 3-yrs, pt survival between the 5 types of IT differed only by 4%; pa survival by 3%; kd survival by 1%.
In group 2 (high-risk), survival rates were significantly higher when IT with depleting agent (TMG/ATG>=4d, were used. Survival was significantly lower when no IT was used or IT with non-depleting or short-term TMG/ATG (<4d) were used. At 3-yrs, pt survival between the 5 types of IT differed by 24%; pa survival by 23% (Figure 1); kd survival by 18%.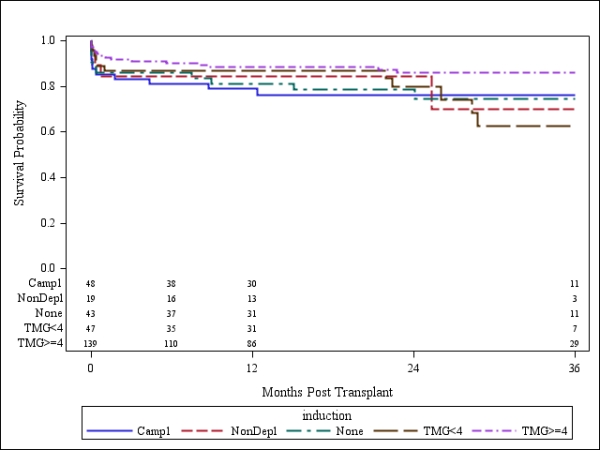
Conclusions: The results were unexpected: in group 1 (low-risk) no significant differences in pt, pa and kd survival were noted between recs without IT or those with maximal IT (>=4d). However, in group 2 (high-risk), overall significantly higher pt, pa and kd survival rates were noted when TMG/ATG>=4d or Campath=1d were used; no IT, non-depleting agents and TMG/ATG<4d resulted in significantly worse survival and should not be used. Thus, for low-risk recs it does not matter if IT and what type of IT is used; however, high-risk recs should receive IT with either TMG/ATG>=4d or Campath>1d for significantly higher pt and graft survival.
To cite this abstract in AMA style:
Gruessner R, Gruessner A. Induction Therapy (IT) in Simultaneous Pancreas and Kidney Transplantation (SPK) according to Patient Risk – A Registry Analysis [abstract]. Am J Transplant. 2015; 15 (suppl 3). https://atcmeetingabstracts.com/abstract/induction-therapy-it-in-simultaneous-pancreas-and-kidney-transplantation-spk-according-to-patient-risk-a-registry-analysis/. Accessed May 29, 2026.« Back to 2015 American Transplant Congress