Incidence of Viral Infections in Kidney Transplant Recipients Using Reduced Induction and Steroid Free Maintenance Immunosuppression
Ohio State University Wexner Medical Center, Columbus, OH
Meeting: 2022 American Transplant Congress
Abstract number: 1003
Keywords: Cytomeglovirus, Induction therapy, Infection, Kidney transplantation
Topic: Clinical Science » Infection Disease » 25 - Kidney Infectious Non-Polyoma & Non-Viral Hepatitis
Session Information
Session Name: Kidney Infectious Non-Polyoma & Non-Viral Hepatitis
Session Type: Poster Abstract
Date: Sunday, June 5, 2022
Session Time: 7:00pm-8:00pm
 Presentation Time: 7:00pm-8:00pm
Presentation Time: 7:00pm-8:00pm
Location: Hynes Halls C & D
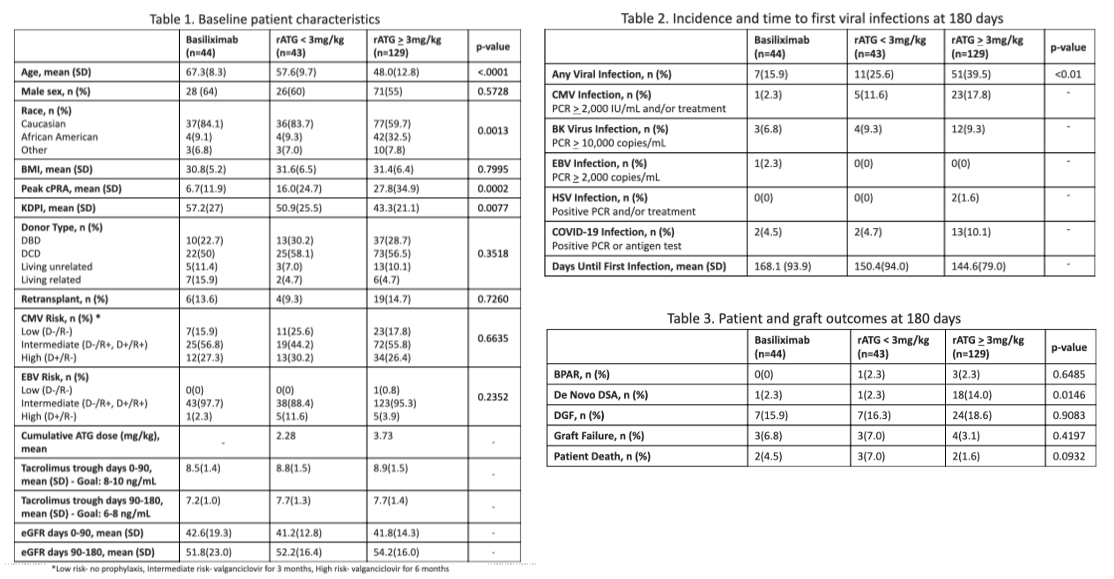
*Purpose: Viral infections (VI) commonly occur in the post-transplant period and higher cumulative doses of rATG have been correlated with higher rates of infection. However, basiliximab (BAS) has decreased risk of infection but increased risk of rejection due to a lower immunosuppressive profile. There is a shortage of literature evaluating choice and dosing of induction agent and the incidence of VI in kidney transplant recipients (KTR) receiving tacrolimus, mycophenolate and early steroid withdrawal. This study evaluated the incidence of VI in KTR receiving BAS, rATG low (< 3mg/kg), or high dose (> 3mg/kg) within 180 days post-transplant.
*Methods: This single-center, retrospective study included adult KTR from July 2020-March 2021. KTR were excluded if they received a multi-organ transplant, no induction, or maintenance immunosuppression other than tacrolimus and mycophenolate. Induction was given based on patients’ immunologic risk factors for rejection which included: age, race, cPRA, retransplantation, and DR HLA mismatch. The primary objective compared the incidence of VI with BAS, rATG low and high dose. Secondary outcomes included incidence of CMV, BKV, EBV, HSV, COVID-19, DGF, BPAR, de novo DSA, eGFR, tacrolimus levels, graft loss, and mortality within 180 days post-transplant.
*Results: There were 44 KTR who received BAS, 43 who received low rATG dose, and 129 who received high rATG dose. Statistically significant differences in baseline demographics included age, race, mean peak cPRA, and mean KDPI (due to institutional induction guidelines) [Table 1]. A larger proportion of high rATG patients experienced VI, followed by low rATG patients, p<0.01 [Table 2]. Increased incidence of CMV, BKV, and COVID-19 occurred in patients receiving rATG [Table 2]. Infections generally occurred earlier in the rATG groups [Table 2]. DSA was highest in the high dose rATG (14%) which was attributed to high risk factors for rejection, p=0.0146 [Table 3]. No differences in BPAR, DGF, graft failure, or mortality were seen between all groups within 180 days.
*Conclusions: KTR that received induction with any rATG dose had a higher incidence of viral infections compared to basiliximab. Induction with rATG may lead to an earlier onset of viral infections compared to basiliximab. Further review of data at one year post-transplant is planned to strengthen the results of this study.
To cite this abstract in AMA style:
Dunton P, Stein LVon, Winters H, Schenk A, Pesavento T, Smith RM, Schnelle K. Incidence of Viral Infections in Kidney Transplant Recipients Using Reduced Induction and Steroid Free Maintenance Immunosuppression [abstract]. Am J Transplant. 2022; 22 (suppl 3). https://atcmeetingabstracts.com/abstract/incidence-of-viral-infections-in-kidney-transplant-recipients-using-reduced-induction-and-steroid-free-maintenance-immunosuppression/. Accessed April 8, 2026.« Back to 2022 American Transplant Congress