Impact Of Nirmatrelvir-Ritonavir On Tacrolimus Concentrations
1University of Rochester Medical Center, Rochester, NY, 2Tampa General Hospital, Tampa, FL
Meeting: 2022 American Transplant Congress
Abstract number: 9053
Keywords: Adverse effects, COVID-19, Drug interaction, Immunosuppression
Topic: Clinical Science » Pharmacy » 29 - Non-Organ Specific: Pharmacokinetics / Pharmacogenomics / Drug interactions
Session Information
Session Time: 7:00pm-8:00pm
 Presentation Time: 7:00pm-8:00pm
Presentation Time: 7:00pm-8:00pm
Location: Hynes Halls C & D
*Purpose: Ritonavir (RTV), a component of the oral antiviral agent nirmatrelvir-RTV (Paxlovid) for COVID-19 infection, increases tacrolimus concentrations through strong competitive inhibition of gastrointestinal and hepatic CYP3A4 enzymes. The prescribing information for nirmatrelvir-RTV recommends against its use in combination with tacrolimus when close monitoring of serum concentrations is not feasible.
*Methods: Herein we report a multicenter case series of 3 patients started on nirmatrelvir-RTV without the knowledge of the transplant team while taking concomitant tacrolimus.
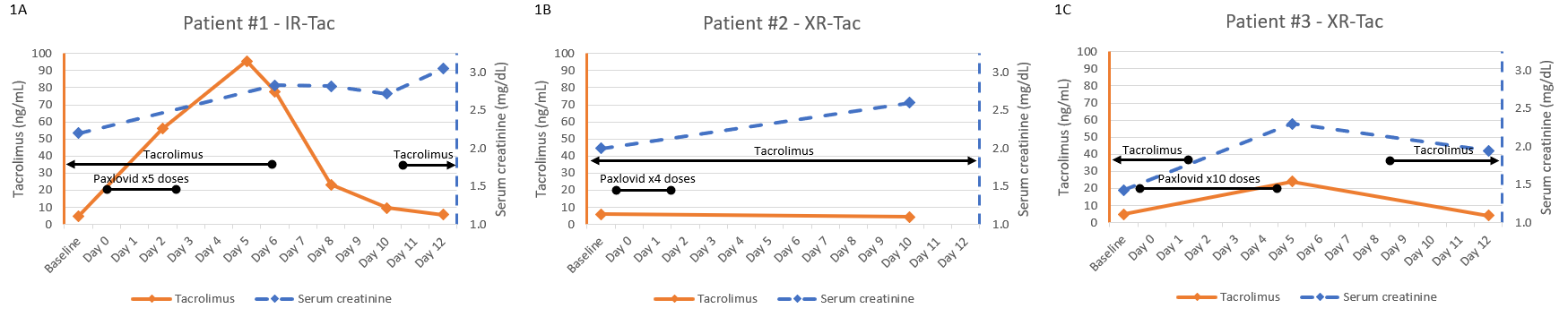
*Results: Figure 1 outlines the time course and lab values for each patient. The first case is a 29 year old male 8 years post-kidney transplant, maintained on immediate release tacrolimus (IR-Tac) (goal 4-6 ng/mL), mycophenolate mofetil (MMF) 500 mg twice daily, and prednisone 5 mg daily. He took 5 doses of nirmatrelvir-RTV before discontinuing due to diarrhea. Six days after his first nirmatrelvir-RTV dose, his tacrolimus level was 95.5 ng/mL and serum creatinine (SCr) 2.8 mg/dL (baseline 2.2 mg/dL). Tacrolimus was discontinued, and 5 days later the level was 9.5 ng/mL. The second case is a 41 year old female 22 years post-kidney transplant, maintained on extended-release tacrolimus (XR-Tac; Envarsus®) (goal 4-6 ng/mL) and prednisone 5 mg daily. She took 4 doses of nirmatrelvir-RTV before discontinuing due to diarrhea and headache, and continued her doses of XR-Tac throughout this time. Ten days after her first nirmatrelvir-RTV dose, her tacrolimus level was 4.4 ng/mL and SCr 2.6 mg/dL (baseline 2.0 mg/dL). The third case is a 66 year old male 1.5 years post-liver transplant, maintained on XR-Tac (goal 4-8 ng/mL) and MMF 500 mg twice daily. He took 4 doses of nirmatrelvir-RTV and then XR-Tac was held while completing nirmatrelvir-RTV therapy. Five days after his first nirmatrelvir-RTV dose and 3 days after his XR-Tac was held, his tacrolimus level was 23.9 ng/mL and SCr 2.4 mg/dL (baseline 1.4 mg/dL).
*Conclusions: In this case series of 3 patients who took nirmatrelvir-RTV while on tacrolimus, duration of nirmatrelvir-RTV and time course of tacrolimus adjustment were variable, and all patients had a rise in SCr from baseline. Given the extreme elevation of tacrolimus concentrations in the patient taking IR-Tac, further study is needed to systematically characterize the variability of this drug interaction between tacrolimus formulations.
To cite this abstract in AMA style:
Fredrick S, Wise B, Bowman L, DeWolfe D, Taylor J, Melaragno J. Impact Of Nirmatrelvir-Ritonavir On Tacrolimus Concentrations [abstract]. Am J Transplant. 2022; 22 (suppl 3). https://atcmeetingabstracts.com/abstract/impact-of-nirmatrelvir-ritonavir-on-tacrolimus-concentrations/. Accessed June 2, 2026.« Back to 2022 American Transplant Congress