Impact of Early Calcineurin-Inhibitor Conversion to Belatacept on Renal Allograft Function in a Steroid-Free Maintenance Regimen: Results from a Randomized Controlled Study
1Northwestern University, Chicago, IL, 2Mount Sinai, New York, NY, 3University of Maryland, Baltimore, MD
Meeting: 2022 American Transplant Congress
Abstract number: 1698
Keywords: Calcineurin, Co-stimulation, Immunosuppression, Kidney transplantation
Topic: Clinical Science » Kidney » 38 - Kidney Immunosuppression: Novel Regimens and Drug Minimization
Session Information
Session Name: Kidney Immunosuppression: Novel Regimens and Drug Minimization
Session Type: Poster Abstract
Date: Tuesday, June 7, 2022
Session Time: 7:00pm-8:00pm
 Presentation Time: 7:00pm-8:00pm
Presentation Time: 7:00pm-8:00pm
Location: Hynes Halls C & D
*Purpose: Belatacept (Bela) was developed to minimize nephrotoxicity and cardiovascular risk associated with Calcineurin inhibitors (CNIs). Early steroid withdrawal (ESW) and simultaneous CNI avoidance (CNIA) using Bela regimen have not been widely evaluated. Here, we evaluated the outcomes of kidney transplant recipients who underwent conversion to Bela immunosuppression with ESW and CNIA at 3 months post-transplant.
*Methods: This is a single-center, prospective, randomized study in which renal allograft recipients received induction with alemtuzumab and maintenance immunosuppressive therapy with tacrolimus (Tac) and mycophenolate (MPA) for the first 3 months post-transplantation. At 3 months, patients were randomized 1:1:1 to conversion to: 1) Bela+MPA, 2) Bela+low-dose Tac (trough goal <5 ng/mL), or 3) continue Tac+MPA. The primary endpoint was the change in eGFR at 2 years post-transplant. The secondary endpoints included patient survival, graft survival, the incidence of biopsy-proven acute rejection (BPAR), and adverse effects. In a subset of 18 patients, we also performed flow cytometric analyses at 3, 6, 12, 18, and 24 months post-transplant.
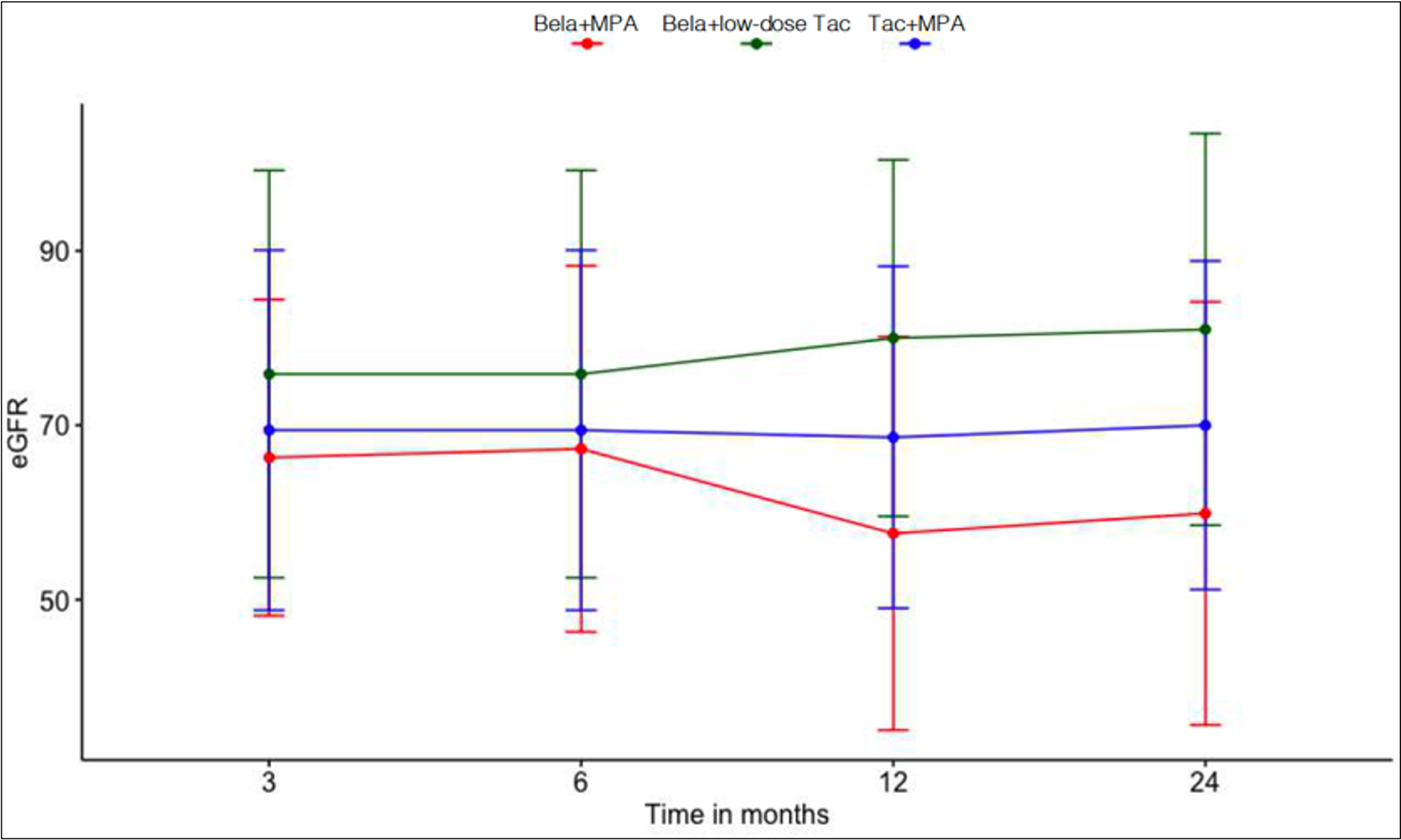
*Results: 27 recipients were included; 9 underwent conversion to Bela+MPA, 8 to Bela+low-dose Tac and 10 continued Tac+MPA. There was no difference in baseline characteristics amongst the 3 groups. The Bela+MPA arm was closed early due to high rate of BPAR. The Bela+low-dose Tac regimen was associated with +8.8 mL/min/1.73 m2 increase in eGFR compared to -0.38 mL/min/1.73 m2 in Tac+MPA, P= 0.243. One graft loss occurred in the Bela+MPA group. [Figure 1]. The incidence of BPAR was 4/9 in Bela+low-dose Tac group, 0/8 in Bela+Tac and 2/10 in Tac+MPA, P= 0.087. Flow cytometric analyses showed no significant differences in effector, anergic, or Treg across groups.
*Conclusions: Conversion to Bela+low dose Tac/ESW improved renal allograft function without causing early rejections, while conversion to Bela +MPA/ESW resulted in high rate of early rejection and lower kidney allograft function or even allograft loss. Further evaluation of Bela with CNIA/ESW in a larger cohort of kidney transplant recipients is needed to support these findings.
To cite this abstract in AMA style:
Tawhari I, Hallak P, Hartzell S, Mas V, Cravedi P, Leventhal J, Ansari J, Gallon L. Impact of Early Calcineurin-Inhibitor Conversion to Belatacept on Renal Allograft Function in a Steroid-Free Maintenance Regimen: Results from a Randomized Controlled Study [abstract]. Am J Transplant. 2022; 22 (suppl 3). https://atcmeetingabstracts.com/abstract/impact-of-early-calcineurin-inhibitor-conversion-to-belatacept-on-renal-allograft-function-in-a-steroid-free-maintenance-regimen-results-from-a-randomized-controlled-study/. Accessed May 25, 2026.« Back to 2022 American Transplant Congress