Illustration of Renal Recovery in SLK with Utilization of Most Recent Allocation Criteria
Henry Ford Hospital Detroit, Detroit, MI
Meeting: 2019 American Transplant Congress
Abstract number: A289
Keywords: Allocation, Ethics, Graft function, Screening
Session Information
Session Name: Poster Session A: Liver - Kidney Issues in Liver Transplantation
Session Type: Poster Session
Date: Saturday, June 1, 2019
Session Time: 5:30pm-7:30pm
 Presentation Time: 5:30pm-7:30pm
Presentation Time: 5:30pm-7:30pm
Location: Hall C & D
*Purpose: Single Center review of Renal recovery in Simultaneous Liver Kidney Transplantation (SLKT) in patients who were approved for SLK based on the recent UNOS criteria. We observed significant increase in renal recovery suggesting ongoing allocation criteria revision. The medical criteria for which recipients would receive a Simultaneous Liver and Kidney Transplant (SLKT) have always been debated. Since kidney function recovery following liver transplantation is difficult to predict, allocation of the kidney for SLKT thus far has not been based on much rationale and evidence. While there are benefits to patients receiving SLKT, kidneys need to be allocated keeping in mind that inappropriate utilization of this scarce resource may be detrimental to the ever-growing population of patients awaiting kidney transplantation.
*Methods: SLK from Jan 2017 until present were evaluated. Of the 14 SLK performed, 4 patients who had dramatic improvement in serum creatinine post operatively were subjected to MAG3 scan for native kidney function assessment.
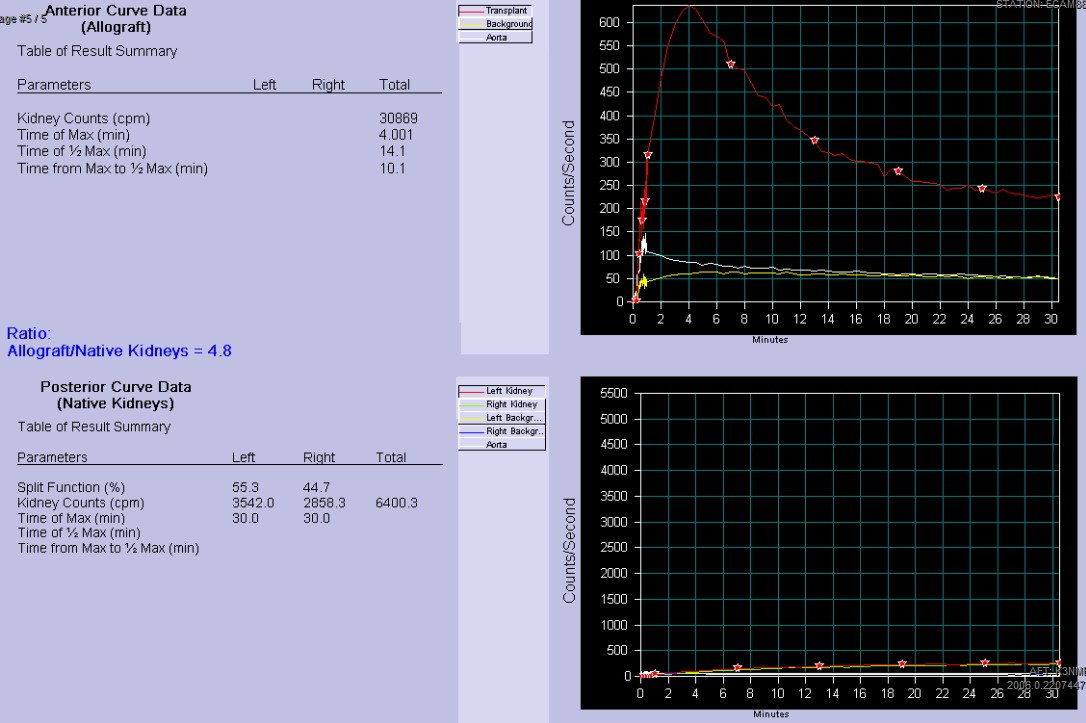
*Results: Our cases here illustrate native kidney recovery and contribution to global assessment of kidney function in SLK. In all cases, MAG3 scan showed activity in native kidneys as well transplanted kidney. Our radiologist provided quantitative analysis of Allograft to Native kidney function in a form of ratio (see table 1). At a glance, the number of native kidney recovery is 4 out of 14 (28%), if we exclude ESRD (based on their dialysis vintage) from this cohort, the percentage of renal recovery becomes 4 out of 9 (44%). Of note, not included in the case series but we incidentally found a patient who underwent SLK in 2006 who was recently evaluated for rejection via MAG3 scan which illustrated all of the renal function provided by Native kidney only
*Conclusions: Although there are benefits to patients with liver and kidney disease receiving SKLT, the biggest downside is that SLKT draw deceased donor kidneys from the kidney transplant candidate pool. Because kidney recovery after liver transplant alone is difficult to predict, indications for SLK cannot be precisely defined. In most of these cases the renal dysfunction may be related to hepatorenal syndrome pathophysiology which could improve significantly following Liver transplant alone(LTA) . The recovery of native kidney function in our case-series underscores an important aspect of this dilemma, as it is because while it would be easy to error on the safe side for the patient by performing an SLKT. Allocating a kidney to a recipient that doesn’t need it, not only deprives another patient of that organ but raises an ethical question for those of KTA waitlist. These patients could be managed by LTA and may benefit from the safety net provision that any LTA recipient who developed ESRD within 1 year of transplant will be listed at the top of the local list for a KDPI 35-100%.
To cite this abstract in AMA style:
Patel B, Prashar R, Babu A. Illustration of Renal Recovery in SLK with Utilization of Most Recent Allocation Criteria [abstract]. Am J Transplant. 2019; 19 (suppl 3). https://atcmeetingabstracts.com/abstract/illustration-of-renal-recovery-in-slk-with-utilization-of-most-recent-allocation-criteria/. Accessed June 3, 2026.« Back to 2019 American Transplant Congress