Hospital Readmissions Following Incompatible Kidney Transplantation: A Multi-Center Study.
Johns Hopkins, Baltimore.
Meeting: 2016 American Transplant Congress
Abstract number: A100
Keywords: Highly-sensitized, Kidney transplantation, Multicenter studies, Post-operative complications
Session Information
Session Name: Poster Session A: Kidney Desensitization
Session Type: Poster Session
Date: Saturday, June 11, 2016
Session Time: 5:30pm-7:30pm
 Presentation Time: 5:30pm-7:30pm
Presentation Time: 5:30pm-7:30pm
Location: Halls C&D
Desensitization and incompatible live donor kidney transplantation (ILDKT) has improved survival vs. forgoing transplant or waiting for a compatible one. It is unknown if increased rejection and infection risks lead to more readmissions than for waitlist candidates or compatible live donor kidney transplant (LDKT) recipients.
Drawing on a 22-center ILDKT cohort, 404 Medicare patients were matched to waitlist controls and LDKT controls on PRA, age, blood group, RRT, number of prior kidney transplants, race, gender, diabetes, and date of addition to the waitlist to the ILDKT transplant date for waitlist matched controls and transplant date for LDKT matched controls. Readmissions were identified using Medicare billing claims. Readmission risk was determined using multilevel, mixed-effects Poisson regression.
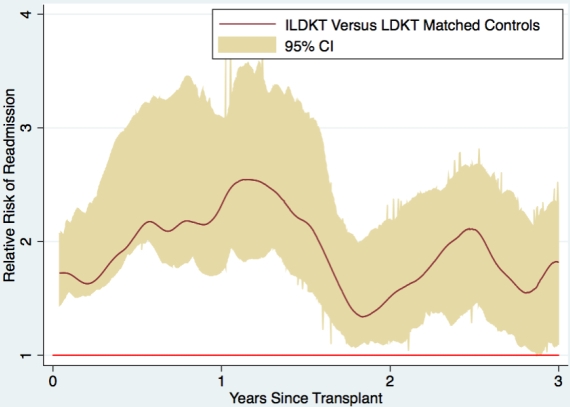
ILDKTs had a readmission risk persistently higher than LDKTs.
|
Relative Risk of Readmission (95%CI) P-Value |
||||
| 0-6 Months | 6 Months-1 Year | 1-2 Years | 2-3 Years | |
| ILDKT vs. LDKT Matched Controls |
1.49 (1.38-1.61) P<0.001 |
1.12 (1.00-1.25) P=0.046 |
1.33 (1.21-1.48) P<0.001 |
1.24 (1.10-1.39) P<0.001 |
| ILDKT vs. Waitlist Matched Controls |
2.37 (2.19-2.58) P<0.001 |
1.60 (1.43-1.80) P<0.001 |
0.78 (0.71-0.86) P<0.001 |
0.72 (0.64-0.80) P<0.001 |
 Compared to waitlist matched controls, ILDKT readmission risk was only higher in the first year (2.37 [95CI:2.19-2.58;P<0.001] from 0- 6 months; 1.60 [95CI:1.43-1.80;P<0.001] in months 6-12); however, thereafter ILDKT recipients had a lower risk compared to waitlist matched controls (0.78 [95CI:0.71-0.86;P<0.001] from years 1-2; 0.72 [95CI:0.64-0.80;P<0.001] from years 2-3).
Compared to waitlist matched controls, ILDKT readmission risk was only higher in the first year (2.37 [95CI:2.19-2.58;P<0.001] from 0- 6 months; 1.60 [95CI:1.43-1.80;P<0.001] in months 6-12); however, thereafter ILDKT recipients had a lower risk compared to waitlist matched controls (0.78 [95CI:0.71-0.86;P<0.001] from years 1-2; 0.72 [95CI:0.64-0.80;P<0.001] from years 2-3).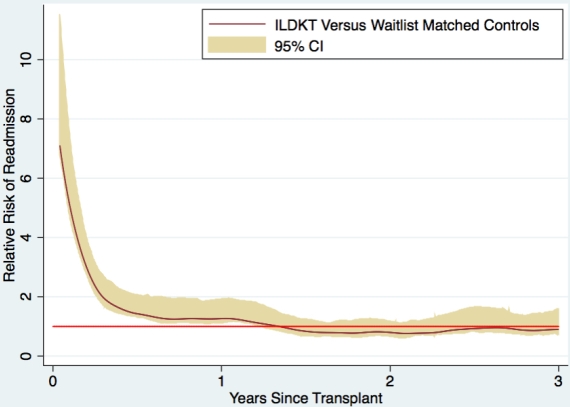
ILDKTs have a higher readmission risk than LDKTs, but a lower readmission risk after the first year post-transplant than waitlist matched controls (and a known survival benefit). These findings should be considered in regulatory/payment schemas.
CITATION INFORMATION: Orandi B, King E, Luo X, Bae S, Lonze B, Montgomery R, Segev D. Hospital Readmissions Following Incompatible Kidney Transplantation: A Multi-Center Study. Am J Transplant. 2016;16 (suppl 3).
To cite this abstract in AMA style:
Orandi B, King E, Luo X, Bae S, Lonze B, Montgomery R, Segev D. Hospital Readmissions Following Incompatible Kidney Transplantation: A Multi-Center Study. [abstract]. Am J Transplant. 2016; 16 (suppl 3). https://atcmeetingabstracts.com/abstract/hospital-readmissions-following-incompatible-kidney-transplantation-a-multi-center-study/. Accessed May 27, 2026.« Back to 2016 American Transplant Congress