Graft Survival in De Novo Donor-Specific Antibodies and Positive Flow Crossmatch Kidney Transplants Is influenced by Class I and Class II.
1Northwestern University Transplant and Outcomes Research Collaborative (NUTORC), Chicago
2Dept of Preventive Medicine, Northwestern University, Chicago
3Astellas Pharma Global Development, Northbrook
4Now with UCB, Atlanta
Meeting: 2017 American Transplant Congress
Abstract number: 52
Keywords: Alloantibodies, HLA antibodies, Kidney transplantation, Survival
Session Information
Session Name: Concurrent Session: Kidney HLA Antibodies
Session Type: Concurrent Session
Date: Sunday, April 30, 2017
Session Time: 2:30pm-4:00pm
 Presentation Time: 3:30pm-3:42pm
Presentation Time: 3:30pm-3:42pm
Location: E354b
Patients with de novo donor-specific antibodies (dnDSA) show inferior graft survival in numerous small studies. We assessed the effect of dnDSA on graft and patient survival in the largest single-center kidney transplant (KT) retrospective cohort to date.
Demographic, laboratory, graft and patient survival data were collected for adult KT patients from 2007–2015. DSA was assessed per protocol at KT (Day 0), 3 and 6 months, 1 and 2 years, and for cause. Continuous variables were summarized by mean (standard deviation; SD) and categorical variables by number/proportion. Kaplan–Meier (KM) method was used to estimate graft and patient survival, with Cox proportional hazards modeling/stepwise variable selection. KM curves were stratified by no dnDSA, dnDSA, and DSA at KT.
Overall, 1517 patients [mean age (SD): 49.5 (13.2), 63.1% male] were followed for ≤8 years (mean 4.4). DSA at KT was associated with 2.42 and 1.89 times greater risk of graft loss and patient death vs no dnDSA, regardless of class/locus. Irrespective of class/locus, overall dnDSA was not associated with increased risk of patient death or graft loss. Stratified for Class I (hazard ratio: 1.6; 95% confidence interval: 1.05, 2.45) and Class II (1.59; 1.04, 2.43), dnDSA were individually associated with increased risk of graft loss, as were human leukocyte antigen (HLA) A, B, DQ and DR. Presence of either DSA at KT was associated with worse graft survival (Figure 1).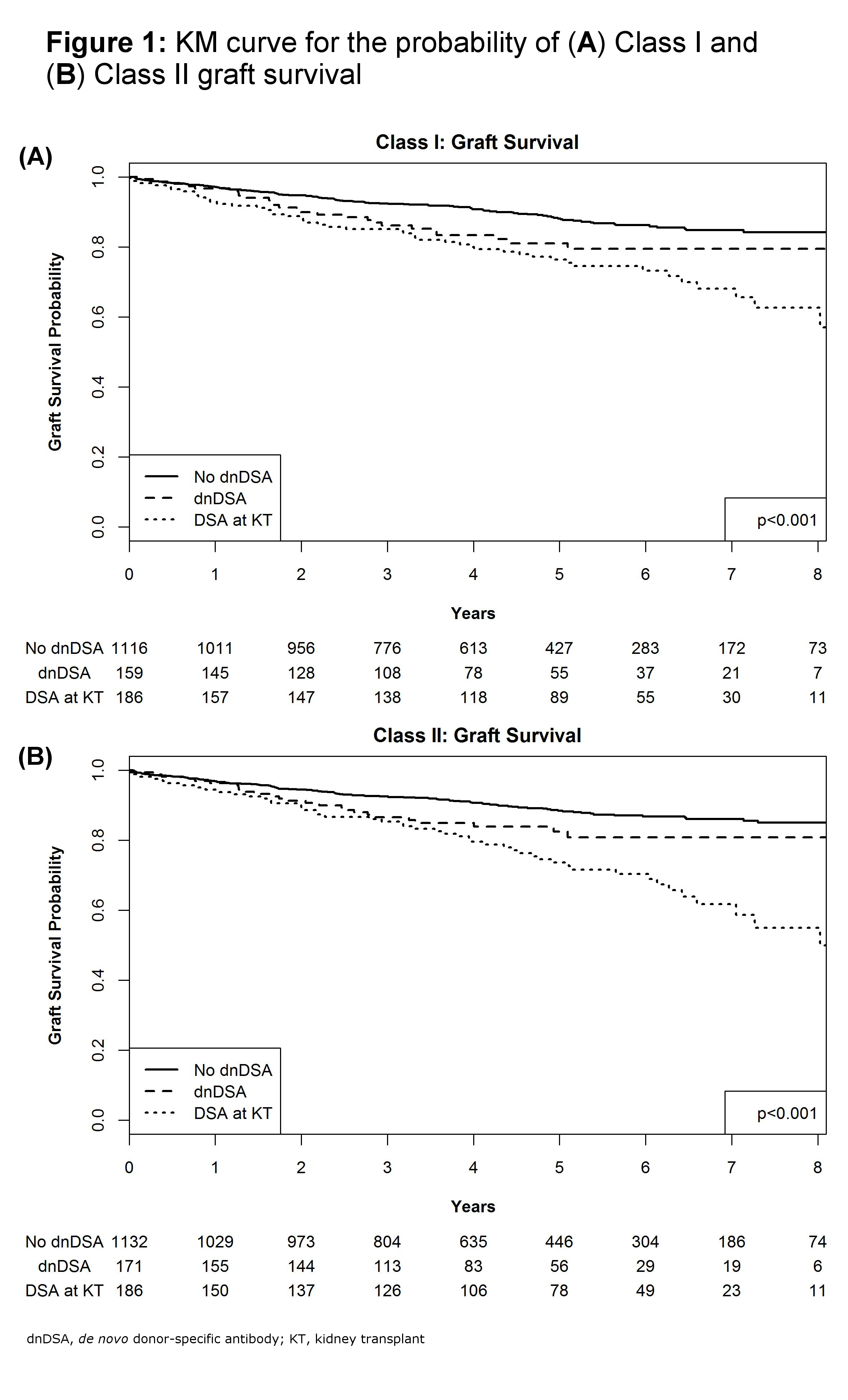 DSA at KT was associated with worse long-term graft and patient survival vs no dnDSA. The emergence of Class I or II dnDSA was associated with increased risk of graft loss, specifically HLA A, B, DQ, and DR.
DSA at KT was associated with worse long-term graft and patient survival vs no dnDSA. The emergence of Class I or II dnDSA was associated with increased risk of graft loss, specifically HLA A, B, DQ, and DR.
CITATION INFORMATION: Montag S, Ho B, Bhagat H, Lee E, Atiemo K, Daud A, Kang R, Zhao L, Schwartz J, Ladner D. Graft Survival in De Novo Donor-Specific Antibodies and Positive Flow Crossmatch Kidney Transplants Is influenced by Class I and Class II. Am J Transplant. 2017;17 (suppl 3).
To cite this abstract in AMA style:
Montag S, Ho B, Bhagat H, Lee E, Atiemo K, Daud A, Kang R, Zhao L, Schwartz J, Ladner D. Graft Survival in De Novo Donor-Specific Antibodies and Positive Flow Crossmatch Kidney Transplants Is influenced by Class I and Class II. [abstract]. Am J Transplant. 2017; 17 (suppl 3). https://atcmeetingabstracts.com/abstract/graft-survival-in-de-novo-donor-specific-antibodies-and-positive-flow-crossmatch-kidney-transplants-is-influenced-by-class-i-and-class-ii/. Accessed May 30, 2026.« Back to 2017 American Transplant Congress