Extreme Hyponatremia as a Risk Factor for Early Mortality After Liver Transplantation in the MELD-Sodium Era
1Division of Transplant and Hepatobiliary Surgery, Henry Ford Hospital, Detroit, MI, 2Division of Gastroenterology and Hepatology, Henry Ford Hospital, Detroit, MI
Meeting: 2021 American Transplant Congress
Abstract number: 1148
Keywords: Allocation, Liver transplantation, Mortality, Waiting lists
Topic: Clinical Science » Liver » Liver: MELD, Allocation and Donor Issues (DCD/ECD)
Session Information
Session Name: Liver: MELD, Allocation and Donor Issues (DCD/ECD)
Session Type: Poster Abstract
Session Date & Time: None. Available on demand.
Location: Virtual
*Purpose: The impact of hyponatremia on waitlist and post-transplant outcomes following the implementation of MELD-Na based liver allocation remains unclear. We sought to evaluate waitlist and post-liver transplant (LT) outcomes in patients with hyponatremia before and after implementation of MELD-Na based allocation.
*Methods: Adult primary LT candidates between 2009 and 2019 were identified in the OPTN/UNOS database. Multi-organ transplants and re-LT were excluded. Two eras were defined: before and after implementation of MELD-Na based allocation. Patients were categorized into the following groups: extreme hyponatremia (≤120 mEq/L), severe hyponatremia (121-124), moderate hyponatremia (125-129), mild hyponatremia (130-134), normal sodium (135-145), and hypernatremia (>145). 90-day waitlist outcomes and post-LT survival were compared according to era and sodium concentration using Fine-Gray and Cox proportional hazard models.
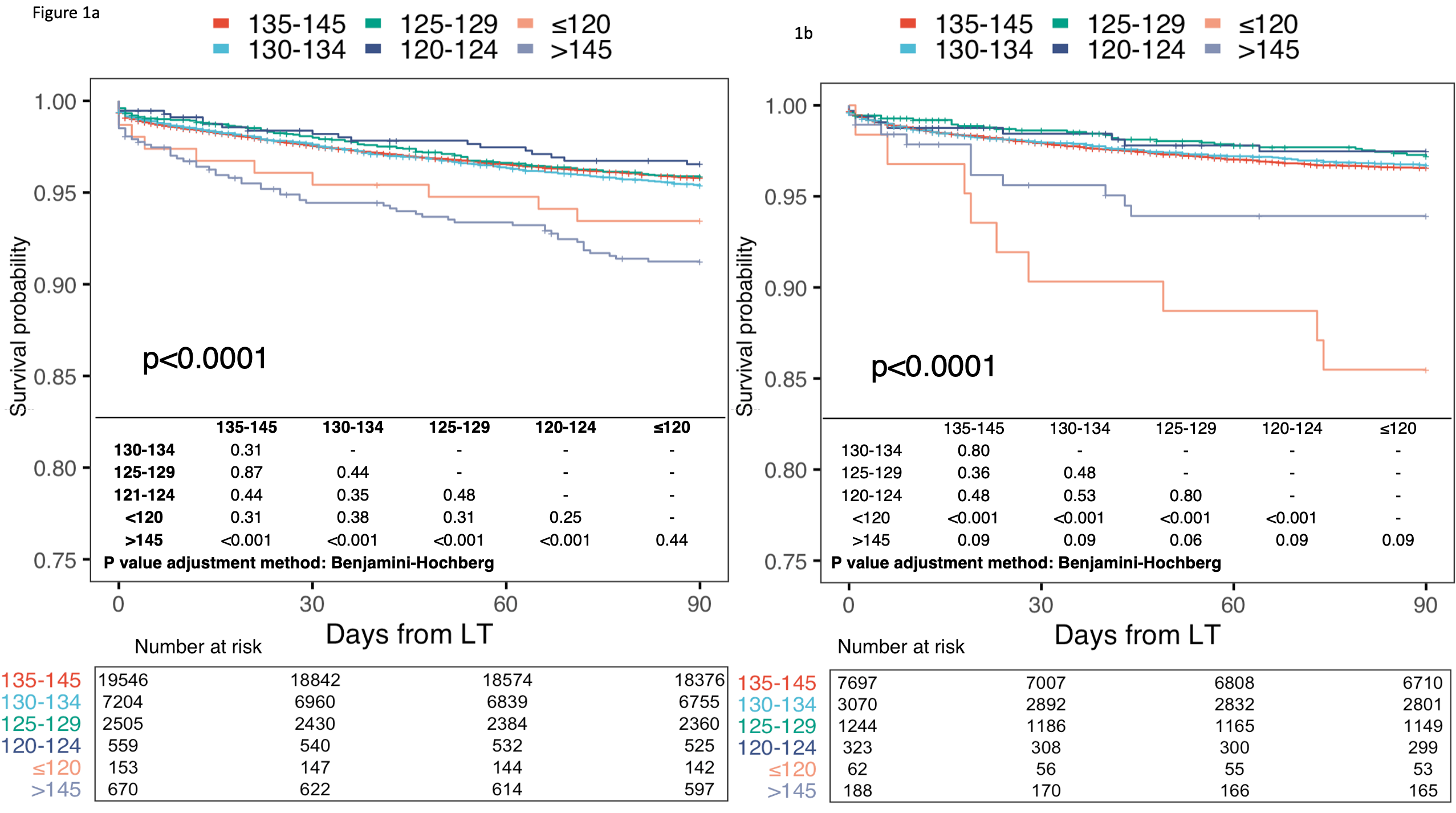
*Results: 87,845 patients were included in waitlist outcome analyses (N=64,911[pre-MELD-Na], N=22,934[post-MELD-Na]). In the pre-MELD-Na era, extreme hyponatremia at listing was associated with increased risk of 90-day waitlist mortality (HR:2.08,p<0.001) and lower likelihood of transplant within 90-days (HR:0.63,p<0.001). In the post-MELD-Na era, patients with extreme hyponatremia had a similar risk of waitlist mortality (HR:1.02,p=0.95) and likelihood of transplant (HR:0.90,p=0.48) as patients with normal serum sodium. Post-LT outcome analyses included 30,639 and 12,585 patients in pre and post-MELD-Na eras. While extreme hyponatremia was not associated with post-LT mortality in the pre-MELD-Na era, it was an independent risk factor for 90-day post-LT mortality in the post-MELD-Na era. (HR:5.20,p<0.001).
*Conclusions: With the introduction of MELD-Na based allocation, waitlist outcomes have improved in patients with extreme hyponatremia but paradoxically been associated with worse short-term post-LT survival.
To cite this abstract in AMA style:
Ivanics T, Leonard-Murali S, Mouzaihem H, Moonka D, Kitajima T, Yeddula S, Shamaa T, Rizzari M, Collins K, Yoshida A, Abouljoud M, Nagai S. Extreme Hyponatremia as a Risk Factor for Early Mortality After Liver Transplantation in the MELD-Sodium Era [abstract]. Am J Transplant. 2021; 21 (suppl 3). https://atcmeetingabstracts.com/abstract/extreme-hyponatremia-as-a-risk-factor-for-early-mortality-after-liver-transplantation-in-the-meld-sodium-era/. Accessed May 15, 2026.« Back to 2021 American Transplant Congress