Eary Use of Statins Associated with Improved Death-Censored Graft Survival Following Kidney Transplant.
1Barnes-Jewish Hospiptal, St. Louis, MO
2Washington University School of Medicine, St. Louis, MO
3St. Louis University, MO.
Meeting: 2016 American Transplant Congress
Abstract number: B228
Keywords: HMG-CoA reductase inhibitor, Kidney transplantation
Session Information
Session Name: Poster Session B: Kidney: Cardiovascular and Metabolic
Session Type: Poster Session
Date: Sunday, June 12, 2016
Session Time: 6:00pm-7:00pm
 Presentation Time: 6:00pm-7:00pm
Presentation Time: 6:00pm-7:00pm
Location: Halls C&D
Purpose: The impacts of statin therapy on patient and graft outcomes after kidney transplantation (KT) are controversial.
Methods: We performed a retrospective cohort study of adult KT recipients at one large center (1999-2014) receiving tacrolimus as their maintenance CNI (defined as prescribed at discharge) and divided them into two groups. Those who were on statin therapy within the month post-transplant versus those that were not on a statin (no statin). Comparisons for death-censored graft survival were made in a multivariable cox-proportional hazards model, including significant predictors for graft loss.
Results: There were 1844 patients with evaluable data during this timeframe, of those 941 were on a statin at month 1 versus 903 patients in the no statin arm. More patients in the statin group received induction with thymoglobulin (89.3% vs. 86.3%, p =0.049) and mycophenolate use was similar (91.1% vs. 89.8%, p=0.357). Graft function (measured by GFR) at 3 months, 6 months, 1 year, and 2 years was similar across groups. Overall, there were 188 death-censored graft losses, and time to death-censored graft loss was similar between groups (44 months vs 40 months, p = 0.451). There was a greater percent of patients surviving in the statin group (92.0% vs. 88.4%, p = 0.008). 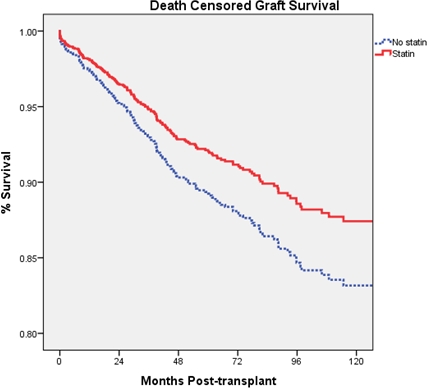 In multivariable analysis, when including age, history of diabetes, hypertension, coronary artery disease, heart failure, HDL, LDL, smoking status, A. Fib, and BMI as covariates, statin exposure remained significant, associated with a 27.0% decreased risk of death-censored graft loss (aHR 0.729, p = 0.038).
In multivariable analysis, when including age, history of diabetes, hypertension, coronary artery disease, heart failure, HDL, LDL, smoking status, A. Fib, and BMI as covariates, statin exposure remained significant, associated with a 27.0% decreased risk of death-censored graft loss (aHR 0.729, p = 0.038).
Conclusion: In a large contemporary sample of KT recipients, early statin use was associated improved death-censored graft survival compared to no exposure or later initiation. Further research into causes of graft loss is warranted.
CITATION INFORMATION: Horwedel T, Brennan D, Lentine K, Hagopian J. Eary Use of Statins Associated with Improved Death-Censored Graft Survival Following Kidney Transplant. Am J Transplant. 2016;16 (suppl 3).
To cite this abstract in AMA style:
Horwedel T, Brennan D, Lentine K, Hagopian J. Eary Use of Statins Associated with Improved Death-Censored Graft Survival Following Kidney Transplant. [abstract]. Am J Transplant. 2016; 16 (suppl 3). https://atcmeetingabstracts.com/abstract/eary-use-of-statins-associated-with-improved-death-censored-graft-survival-following-kidney-transplant/. Accessed May 23, 2026.« Back to 2016 American Transplant Congress