Combination of Delayed Kidney Transplant (KT) and Better Quality Kidneys Offers Excellent Patient Survival in Combined Liver-Kidney Transplantation (CLKT).
Transplant Division, Department of Surgery, Indiana University, Indianapolis, IN.
Meeting: 2016 American Transplant Congress
Abstract number: 76
Keywords: Kidney transplantation, Kidney/liver transplantation, Liver transplantation, Outcome
Session Information
Session Name: Concurrent Session: The Kidney in Liver Transplantation
Session Type: Concurrent Session
Date: Sunday, June 12, 2016
Session Time: 2:30pm-4:00pm
 Presentation Time: 2:30pm-2:42pm
Presentation Time: 2:30pm-2:42pm
Location: Room 302
Background: Despite prioritizing high MELD patients with the share-35 policy, patient survival in CLKT is relatively low. We previously showed the positive impact of delayed KT on patient survival in CLKT, offering a less hostile environment with hemodynamically more stable patient at the time of KT. The purpose of this study is to identify whether the quality of kidneys (based on KDPI) or the delayed approach KT prolongs patient survival. Methods: 130 CLKT were performed between 2002-2015 at Indiana University. All kidneys underwent continuous hypothermic pulsatile perfusion until KT; 69 with simultaneous KT (at time of LT, Group S) and 61 with delayed KT (Group D) (performed at a later time as a second operation, mean CIT of 50±15h). All patients were categorized according to the KDPI score; 1-33%, 34-66%, and 67-99%. Outcomes for patients in Groups S and D were then compared by KDPI. All patients received the same immunosuppression and continuous veno-venous hemodialysis during the LT, which was continued until KT. Results: Recipient and donor characteristics were comparable within Groups S and D, including recipient age, BMI, MELD, Hepatitis C status, pre-KT dialysis and its duration. The higher KDPI groups had higher donor age, more ECD kidneys, and more deaths due to stroke, as expected. Transplant outcomes were comparable within Groups S and D, liver and kidney CIT and WIT, DGF rate, transfusion and pressor requirements, and ICU stays. Low KDPI kidneys are associated with increased patient survival in both groups. Delayed approach KT resulted in no DGF in Group D and prolonged patient survival >10% in each subgroups compared to Group S 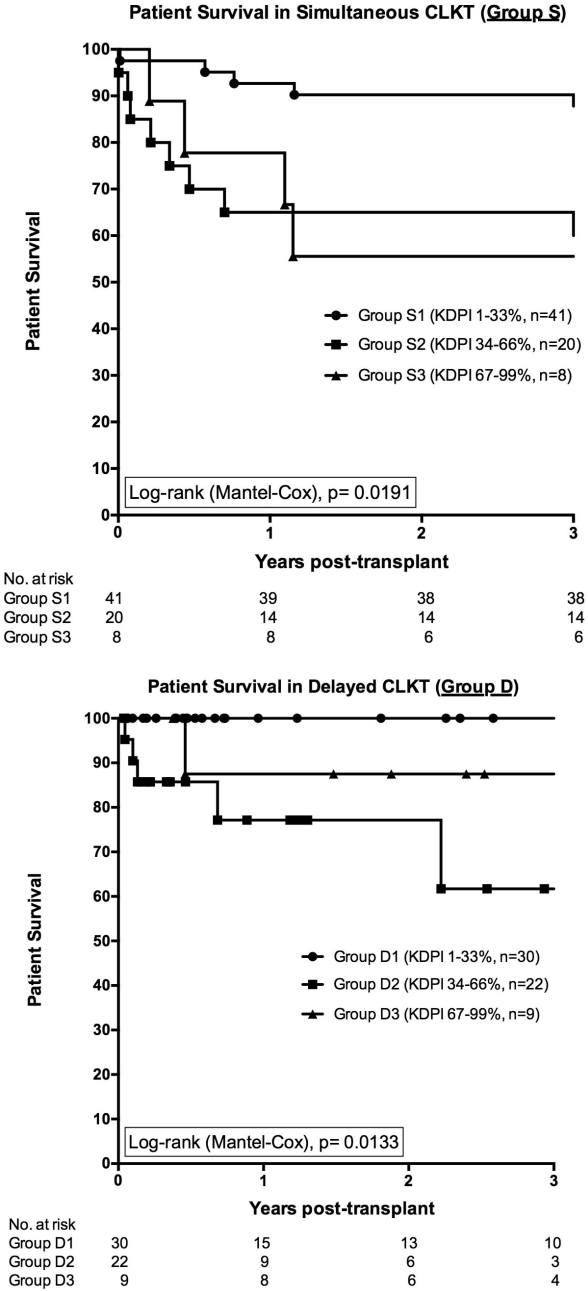 . Conclusion: These results support that the delayed KT in CLKT; (i) should be the preferred method regardless of the KDPI of the renal graft; (ii) if combined with the use of better quality kidneys offers excellent patient survival up to 3 years; and (iii) helps expanding the donor pool with the use of more ECD and DCD kidneys with similar outcomes.
. Conclusion: These results support that the delayed KT in CLKT; (i) should be the preferred method regardless of the KDPI of the renal graft; (ii) if combined with the use of better quality kidneys offers excellent patient survival up to 3 years; and (iii) helps expanding the donor pool with the use of more ECD and DCD kidneys with similar outcomes.
CITATION INFORMATION: Ekser B, Mangus R, Fridell J, Kubal C, Bayt D, Nagaraju S, Mihaylov P, Powelson J, Goggins W, Tector A. Combination of Delayed Kidney Transplant (KT) and Better Quality Kidneys Offers Excellent Patient Survival in Combined Liver-Kidney Transplantation (CLKT). Am J Transplant. 2016;16 (suppl 3).
To cite this abstract in AMA style:
Ekser B, Mangus R, Fridell J, Kubal C, Bayt D, Nagaraju S, Mihaylov P, Powelson J, Goggins W, Tector A. Combination of Delayed Kidney Transplant (KT) and Better Quality Kidneys Offers Excellent Patient Survival in Combined Liver-Kidney Transplantation (CLKT). [abstract]. Am J Transplant. 2016; 16 (suppl 3). https://atcmeetingabstracts.com/abstract/combination-of-delayed-kidney-transplant-kt-and-better-quality-kidneys-offers-excellent-patient-survival-in-combined-liver-kidney-transplantation-clkt/. Accessed June 1, 2026.« Back to 2016 American Transplant Congress