Chronic Active T-Cell Mediated Rejection is Variably Responsive to Immunosuppressive Therapy
1Pathology, Cedars-Sinai Medical Center, Los Angeles, CA, 2Comprehensive Transplant Center, Cedars-Sinai Medical Center, Los Angeles, CA
Meeting: 2020 American Transplant Congress
Abstract number: D-056
Keywords: Fibrosis, Histology, Kidney transplantation, Rejection
Session Information
Session Name: Poster Session D: Kidney: Acute Cellular Rejection
Session Type: Poster Session
Date: Saturday, May 30, 2020
Session Time: 3:15pm-4:00pm
 Presentation Time: 3:30pm-4:00pm
Presentation Time: 3:30pm-4:00pm
Location: Virtual
*Purpose: Chronic active T cell-mediated rejection (CACMR) is a newly described variant of kidney allograft rejection associated with long-term graft loss. A key histologic feature of CACMR is inflammation in areas of interstitial fibrosis and tubular atrophy (i-IFTA). Whether i-IFTA is related to underimmunosuppression is debated and the benefit of immunosuppressive therapy in CACMR is unknown. Here we investigate the amenability of CACMR to treatment and examine the impact of histologic parameters and donor derived cell free DNA (dd-cfDNA, Allosure, CareDx, Inc.) on outcomes.
*Methods: We performed a retrospective single institution review for diagnoses of isolated CACMR 1A or 1B in allograft biopsies. dd-cfDNA levels at the time of biopsy, if and how patients were treated, and the association of dd-cfDNA and treatment with eGFR over time was assessed. Complete response was defined as a return to ≥90% of baseline eGFR, and partial response as a ≥40% recovery of eGFR.
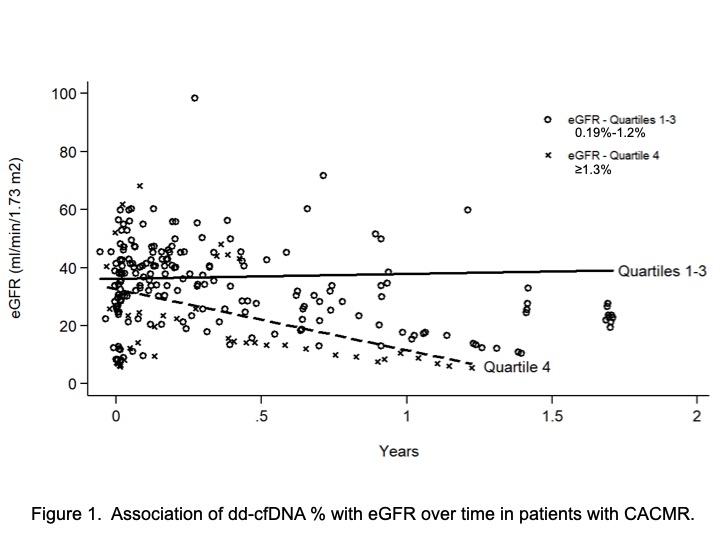
*Results: 51 unique cases of CACMR were identified. Of these, 31 were associated with ≥10 ml/min/1.73 m2 decline in eGFR from baseline, of which 29 were treated and 2 untreated. The most common treatment was pulse steroids (21/31), followed by anti-thymocyte globulin (ATG) (8/31). Neither untreated case had improvement in graft function. Of steroid-treated cases, 10/21 (48%) had a partial (7/21) or complete (3/21) response at 2 weeks post treatment. Among ATG-treated cases, 2/8 (25%) had a partial response and none a complete response. Of 8 treated responders with 3-month follow-up, 4 had sustained response. Neither CACMR grade (t score), IFTA (ci + ct scores), or Banff i score was significantly associated with treatment response. A subgroup of 19/51 patients had assessment of dd-cfDNA within 30 days of biopsy. Using a linear mixed effects model, dd-cfDNA≤1.2% was associated with stable eGFR [eGFR slope: 1.6 (-6.9 to 10.2) ml/min/1.73 m2/year] whereas dd-cfDNA≥1.3% was associated with eGFR decline over time [slope: -21.1 (-39.9 to -2.2) ml/min/1.73 m2/year; p for interaction 0.03] (Figure 1).
*Conclusions: CACMR is not a homogenous entity. In a subset of cases, sustained improvement in renal function can be achieved by pulse steroid or ATG treatment. The features rendering steroids or ATG ineffective in other cases have yet to be identified, although dd-cfDNA may be a potential prognostic indicator. Ongoing efforts are focused on establishing a molecular signature of CACMR that might be used in concert with histopathology to determine treatment responsiveness.
To cite this abstract in AMA style:
Kung V, Haas M, Gillespie M, Huang E, Sandhu R. Chronic Active T-Cell Mediated Rejection is Variably Responsive to Immunosuppressive Therapy [abstract]. Am J Transplant. 2020; 20 (suppl 3). https://atcmeetingabstracts.com/abstract/chronic-active-t-cell-mediated-rejection-is-variably-responsive-to-immunosuppressive-therapy/. Accessed March 21, 2026.« Back to 2020 American Transplant Congress