An Interventional Study Using Cell-Mediated Immunity to Guide Primary Prophylaxis for CMV Infection in Organ Transplant Recipients: A Multi-Center Study
1UHN, Toronto, ON, Canada, 2UAlberta, Edmonton, AB, Canada, 3UBC, Vancouver, BC, Canada, 4LHSC, London, ON, Canada, 5StMH, Toronto, ON, Canada
Meeting: 2022 American Transplant Congress
Abstract number: 52
Keywords: Cytomeglovirus, Interferon (IFN), Prophylaxis, T cell reactivity
Topic: Clinical Science » Infection Disease » 24 - All Infections (Excluding Kidney & Viral Hepatitis)
Session Information
Session Name: Cytomegalovirus and other Herpes Viruses
Session Type: Rapid Fire Oral Abstract
Date: Sunday, June 5, 2022
Session Time: 3:30pm-5:00pm
 Presentation Time: 3:50pm-4:00pm
Presentation Time: 3:50pm-4:00pm
Location: Hynes Ballroom B
*Purpose: There are limited interventional studies using CMV cell-mediated immunity to guide the duration of antiviral prophylaxis. We aimed to use CMV CMI to guide primary CMV prophylaxis in organ transplant recipients at high risk of CMV.
*Methods: We performed a single-arm prospective multicenter study including kidney, pancreas, liver, and heart transplant recipients who were eligible to receive antiviral prophylaxis for CMV for either (i) D+/R- serostatus or (ii) R+ status with anti-thymocyte globulin induction. CMV CMI (Quantiferon-CMV) was performed at post-transplant months 3,4,5 and prophylaxis was discontinued for a positive result but continued for a negative result up to a maximum of 6 months. Patients were monitored for CMV viremia and CMV disease up to 1 year post-transplant. The primary endpoint was CMV viremia >=1000 IU/mL.
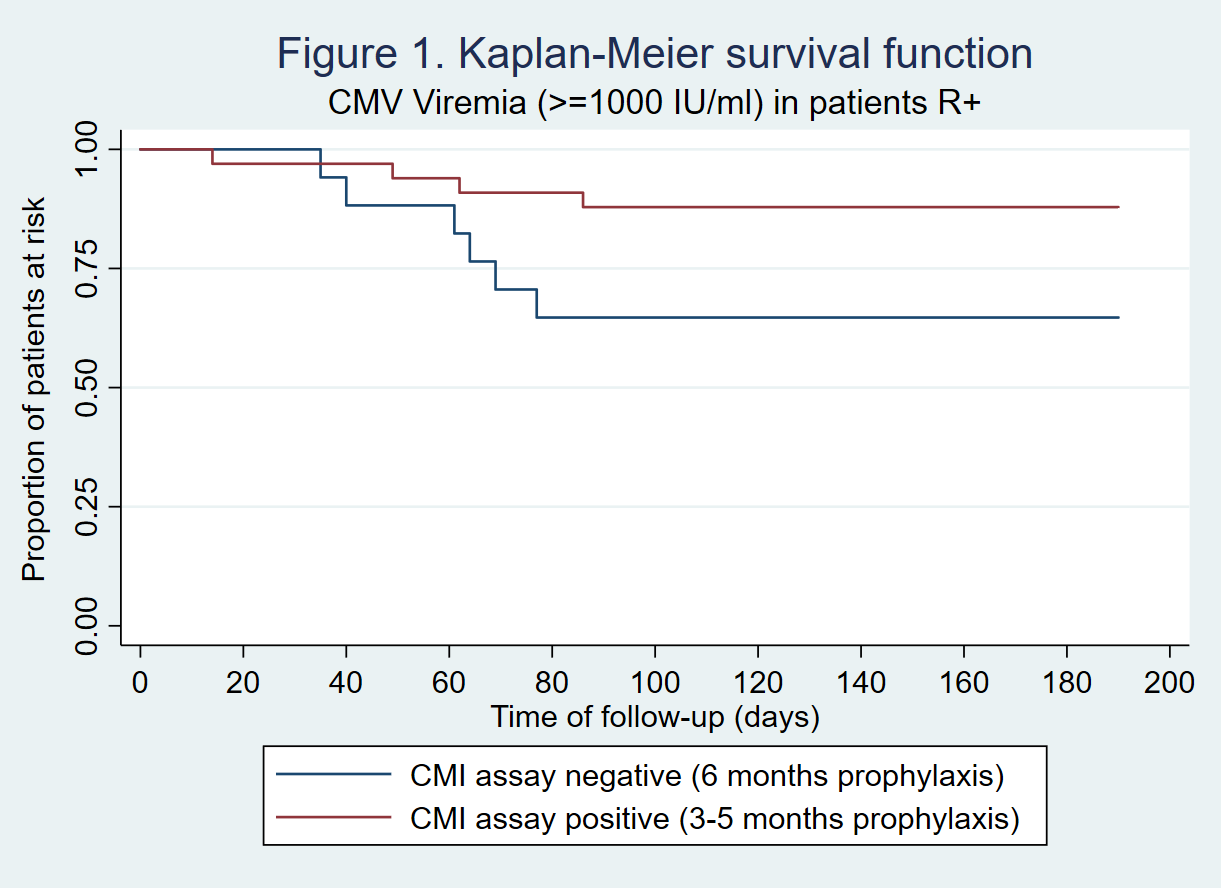
*Results: A total of 108 patients were included. 62% were males and mean age was 53.1 years (SD 13.3). Transplant types were kidney (n=89), kidney-pancreas (n=7), liver (n=10), and heart (n=2). 12% had a previous transplant. CMV serologic status was D+/R- in 48 patients (44.4%) and R+ in 60 patients (55.6%). Of these, 89 patients (82.4%) completed the follow-up period (n=39 D+/R- and n=50 R+). In the D+/R- group, only 1/39 (2.6%) had a positive CMV CMI prior to 6 months and discontinued prophylaxis early. During followup of D+/R- patients,15/38 (39.5%) CMI negative patients developed CMV viremia over 1000 IU/mL, and 5(13.2%) had CMV disease. Two patients (5.1%) had biopsy-proven rejection and 6 (15.4%) had significant leukopenia. In the R+ group, 33/50 (66%) had a positive CMI assay prior to 6 months: 28 at month 3 post-transplant, 4 at month 4, and 1 at month 5. During followup, CMV viremia >=1000 IU/mL occurred in only 4/33 (12.1%) patients that discontinued prophylaxis early and in 6/17 (35.3%) of patients that were CMI negative and continued prophylaxis till 6 months (p=0.14) (Figure 1). No R+ patient developed CMV disease. There were no significant differences in hematologic adverse effects between early discontinuation and extended 6 month prophylaxis in the R+ group.
*Conclusions: CMV CMI guided prophylaxis does not appear to be useful in D+/R- patients since the vast majority do not develop a positive CMI while on antiviral prophylaxis. However, guided prophylaxis appears useful in R+ patients who may benefit from extension of prophylaxis or close monitoring if CMI negative.
To cite this abstract in AMA style:
Solera JT, Cervera C, Hosseini S, Gill J, Shalhoub S, Zaltzman J, Pinzon N, Humar A, Kumar D. An Interventional Study Using Cell-Mediated Immunity to Guide Primary Prophylaxis for CMV Infection in Organ Transplant Recipients: A Multi-Center Study [abstract]. Am J Transplant. 2022; 22 (suppl 3). https://atcmeetingabstracts.com/abstract/an-interventional-study-using-cell-mediated-immunity-to-guide-primary-prophylaxis-for-cmv-infection-in-organ-transplant-recipients-a-multi-center-study/. Accessed April 7, 2026.« Back to 2022 American Transplant Congress