Association Of Lymphocyte-depleting Antibody And Steroids Induction With The Risk And Outcomes Of Post-transplant Diabetes: Analysis Of Deceased-donor Kidney Transplants
1Div. of Nephrology, Hypertension & Renal Transplantation, University of Florida, Gainesville, FL, 2University of Florida, Gainesville, FL, 3Ubon Ratchathani University, Ubonratchathani, Thailand
Meeting: 2019 American Transplant Congress
Abstract number: 560
Keywords: Graft failure, Induction therapy, Kidney transplantation, Post-transplant diabetes
Session Information
Session Name: Concurrent Session: Kidney Immunosuppression: Induction Therapy
Session Type: Concurrent Session
Date: Tuesday, June 4, 2019
Session Time: 4:30pm-6:00pm
 Presentation Time: 5:06pm-5:18pm
Presentation Time: 5:06pm-5:18pm
Location: Room 304
*Purpose: We aimed to determine the risk and outcomes of post-transplant diabetes(PTDM) associated with combined lymphocyte-depleting antibody (LDA) [anti-thymocyte globulin (ATG) or alemtuzumab (ALM)] and steroids induction in adult deceased-donor (DD) kidney transplant (KT) recipients (KTRs).
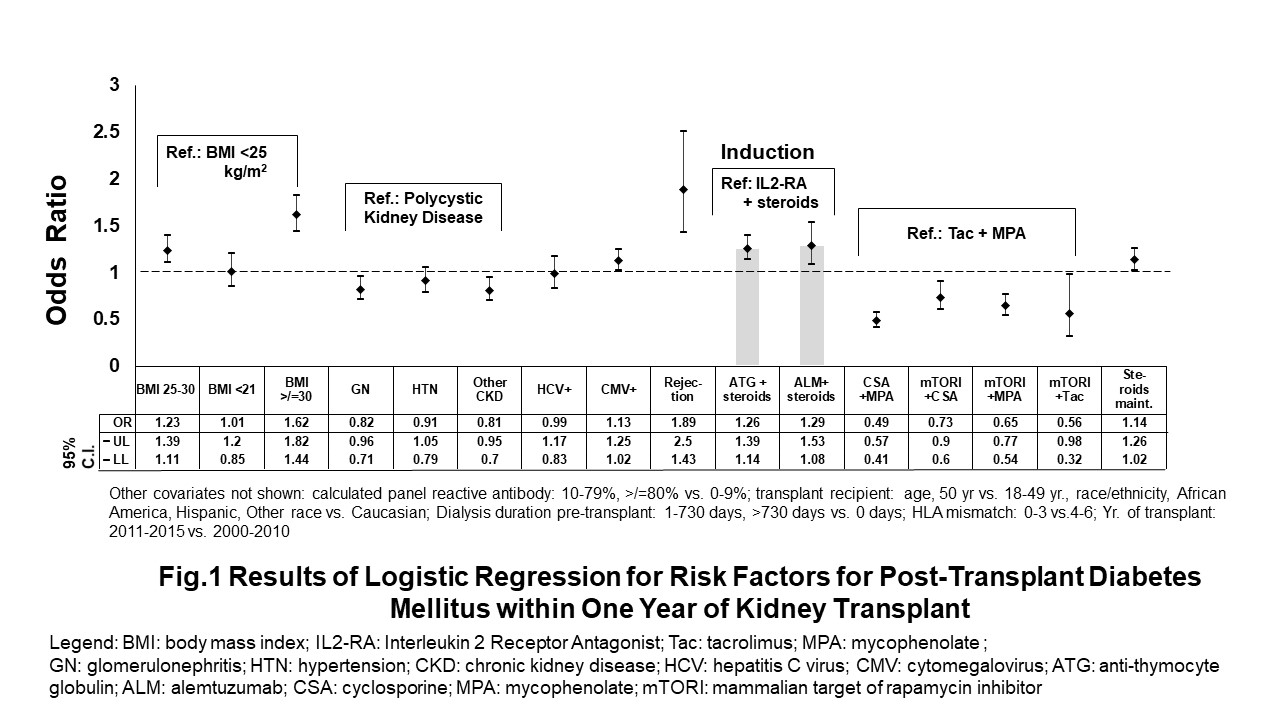
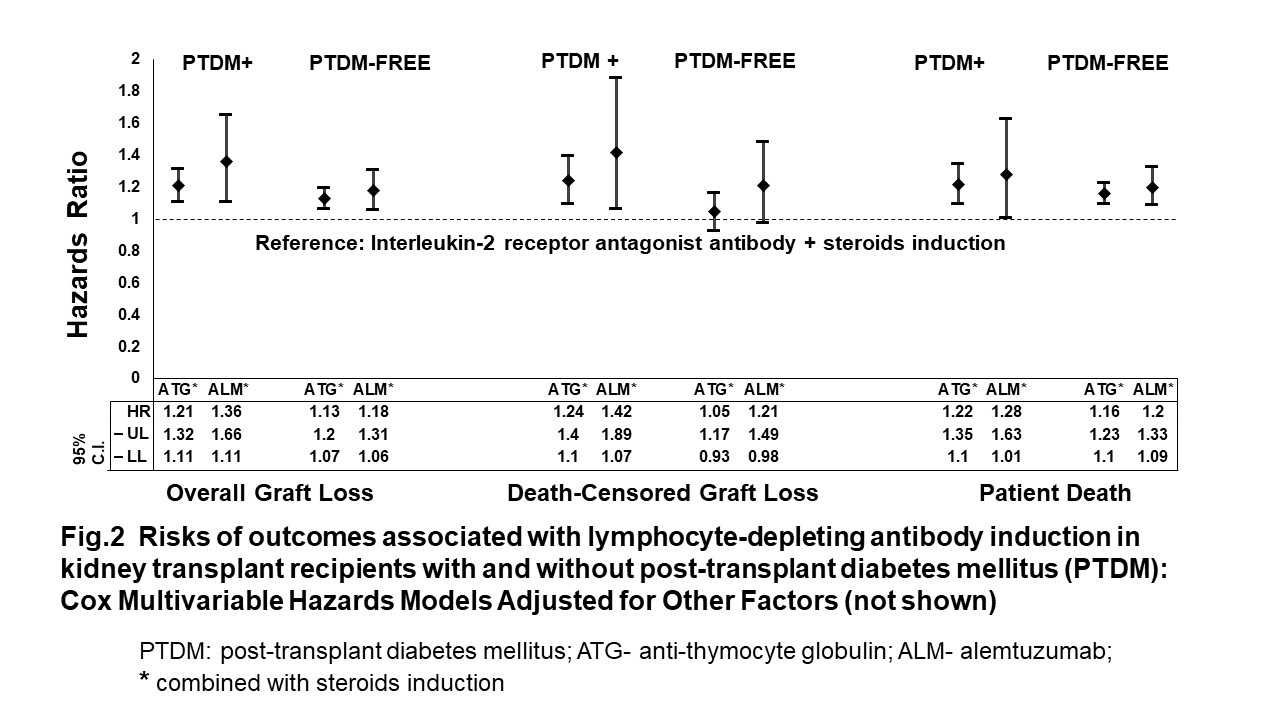
*Methods: From 12/5/2007-7/16/2015 OPTN data, we used logistic regression to analyze the risk factors for PTDM at one-year post-kidney transplant with LDA+steroids induction regimens (ATG+steroids and ALM+steroids) as main explanatory variables and interleukin-2 receptor antagonist+steroids (IL2-RA+steroids) as reference. We used Cox regression models to determine the 5-year risks of overall graft loss (OAGL), death-censored graft loss (DCGL) and patient death (mortality) associated with LDA+steroids regimens in KTR with and without PTDM.
*Results: : ATG+steroids and ALM+steroids were associated with 26% and 29% higher odds ratios of PTDM, respectively than IL2-RA +steroids at 1-year post-KT [Fig. 1]. Other significant risks factors of PTDM were: panel reactive antibody>/=80%, body mass index (25-29 and >/=30 kg/m2), KTR race, dialysis duration, HLA mismatch>3, CMV+ serology, maintenance steroids and acute rejection episodes [Fig. 1]. The risks of 5-year OAGL and mortality associated with ATG+steroids or ALM+steroids (vs. IL2-RA+steroids) induction did not differ between KTRs with and without PTDM at 1-year post-transplant [Fig. 2]. However, the risk of 5-year DCGL was higher in KTR who received ATG+steroids induction and developed PTDM at 1-year post-transplant compared with KTR who received ATG+steroids induction but were PTDM-free at 1-year post-transplant [Fig. 2].
*Conclusions: In adult DD-KTRs, 1-year PTDM risk is higher with lymphocyte-depleting antibody with steroids vs. IL2-RA with steroids induction. LDA+steroids induction is a significant risk factor for death-censored graft loss in KTR with PTDM, not in KTR free of PTDM at 1-year post-transplant.
To cite this abstract in AMA style:
Santos A, Gregg J, Akanit UL, Alquadan K, Bejjanki H, Womer KL. Association Of Lymphocyte-depleting Antibody And Steroids Induction With The Risk And Outcomes Of Post-transplant Diabetes: Analysis Of Deceased-donor Kidney Transplants [abstract]. Am J Transplant. 2019; 19 (suppl 3). https://atcmeetingabstracts.com/abstract/association-of-lymphocyte-depleting-antibody-and-steroids-induction-with-the-risk-and-outcomes-of-post-transplant-diabetes-analysis-of-deceased-donor-kidney-transplants/. Accessed May 23, 2026.« Back to 2019 American Transplant Congress