Variation in Cost of Death and Graft Failure across All Solid Organs
1St. Louis Univ, St. Louis, MO
2SRTR, Minneapolis, MN
3Lahey Hosp & Med Ctr, Burlington, VT.
Meeting: 2018 American Transplant Congress
Abstract number: 474
Keywords: Economics, Graft survival, Survival
Session Information
Session Name: Concurrent Session: Non-Organ Specific: Economics, Public Policy, Allocation, Ethics - 2
Session Type: Concurrent Session
Date: Tuesday, June 5, 2018
Session Time: 2:30pm-4:00pm
 Presentation Time: 2:42pm-2:54pm
Presentation Time: 2:42pm-2:54pm
Location: Room 4C-4
Medicare costs for transplant vary considerably by organ, and costs in the second posttransplant year (Y2) are lower than in the first (Y1). Variability in costs by posttransplant outcome are less well known.
Using SRTR data linked to Medicare claims, we summarized posttransplant Medicare expenditures for transplants in Y1 and Y2 by organ and posttransplant outcomes. We computed Y1 costs for recipients in 2008-2013, for whom Medicare was the primary payer at transplant. The Y2 cohort was similar, with transplant dates 2008-2012. For costs by outcome, we attributed all costs in the year to the outcome of interest; if death-censored graft failure (DCGF) occurred any time in Y2, all Y2 costs were attributed to DCGF.
In Y1, overall costs varied from $82K for kidney recipients to $366K for intestine recipients. For recipients of all organs, functioning grafts were less costly than death or graft failure. For kidney recipients, DCGF was 4.3 times more costly than functioning grafts, likely due to the high cost of dialysis. Death was 4.7 times more costly than functioning grafts. For liver recipients, Medicare paid 2.5 times more for DCG and re-transplants, and 4.8 times more for death than for functioning grafts. For heart and lung recipients, the cost of dying in the first year was 4.5 and 3.9 times more than for functioning grafts.
In Y2, overall costs varied from $26K for kidney recipients to $105K for intestine recipients. The cost difference between functioning and failed grafts was more extreme for most organs. For kidney recipients, DCGF was 9 times more costly and death nearly 5.9 times more costly than functioning grafts. For liver recipients, Medicare paid 4.9 times more for DCGF and 5.8 times more for death than for functioning grafts. For lung recipients, DCGF was more costly than death, 6.4 vs. 4.8 times the cost of functioning grafts.
Costs of death and graft failure are high after solid organ transplant. This information is essential for determining the value of interventions designed to avoid these outcomes. These data can facilitate efforts to improve outcomes across all solid organ transplant types.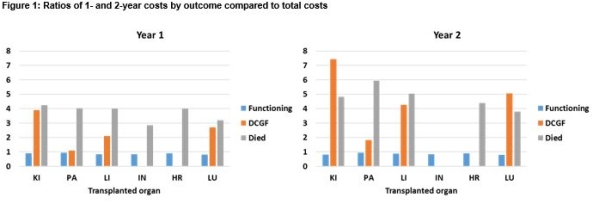
CITATION INFORMATION: Schnitzler M., Skeans M., Axelrod D., Lentine K., Randall H. Variation in Cost of Death and Graft Failure across All Solid Organs Am J Transplant. 2017;17 (suppl 3).
To cite this abstract in AMA style:
Schnitzler M, Skeans M, Axelrod D, Lentine K, Randall H. Variation in Cost of Death and Graft Failure across All Solid Organs [abstract]. https://atcmeetingabstracts.com/abstract/variation-in-cost-of-death-and-graft-failure-across-all-solid-organs/. Accessed March 30, 2026.« Back to 2018 American Transplant Congress