Variation Exists in Hospital Policies for Donation After Circulatory Death Within a Single Donor Service Area
1Baylor University Medical Center, Dallas, TX, 2Texas A&M University College of Medicine, Dallas, TX, 3Southwest Transplant Alliance, Dallas, TX
Meeting: 2022 American Transplant Congress
Abstract number: 1334
Keywords: Circulatory Death, Donors, non-heart-beating, Ethics, Public policy
Topic: Clinical Science » Public Policy » 21 - Non-Organ Specific: Public Policy & Allocation
Session Information
Session Name: Non-Organ Specific: Public Policy & Allocation
Session Type: Poster Abstract
Date: Monday, June 6, 2022
Session Time: 7:00pm-8:00pm
 Presentation Time: 7:00pm-8:00pm
Presentation Time: 7:00pm-8:00pm
Location: Hynes Halls C & D
*Purpose: The Joint Commission mandates that all hospitals have a donation after circulatory death (DCD) policy. Previous studies have demonstrated variability in DCD policy elements. With the increasing utilization of DCD donors, we hypothesized that there would be more consistency among DCD policies.
*Methods: Deidentified DCD hospital policies from the Southwest Transplant Alliance (STA) DSA were collected. Two researchers extracted policy elements and descriptive and bivariate statistical analysis was performed.
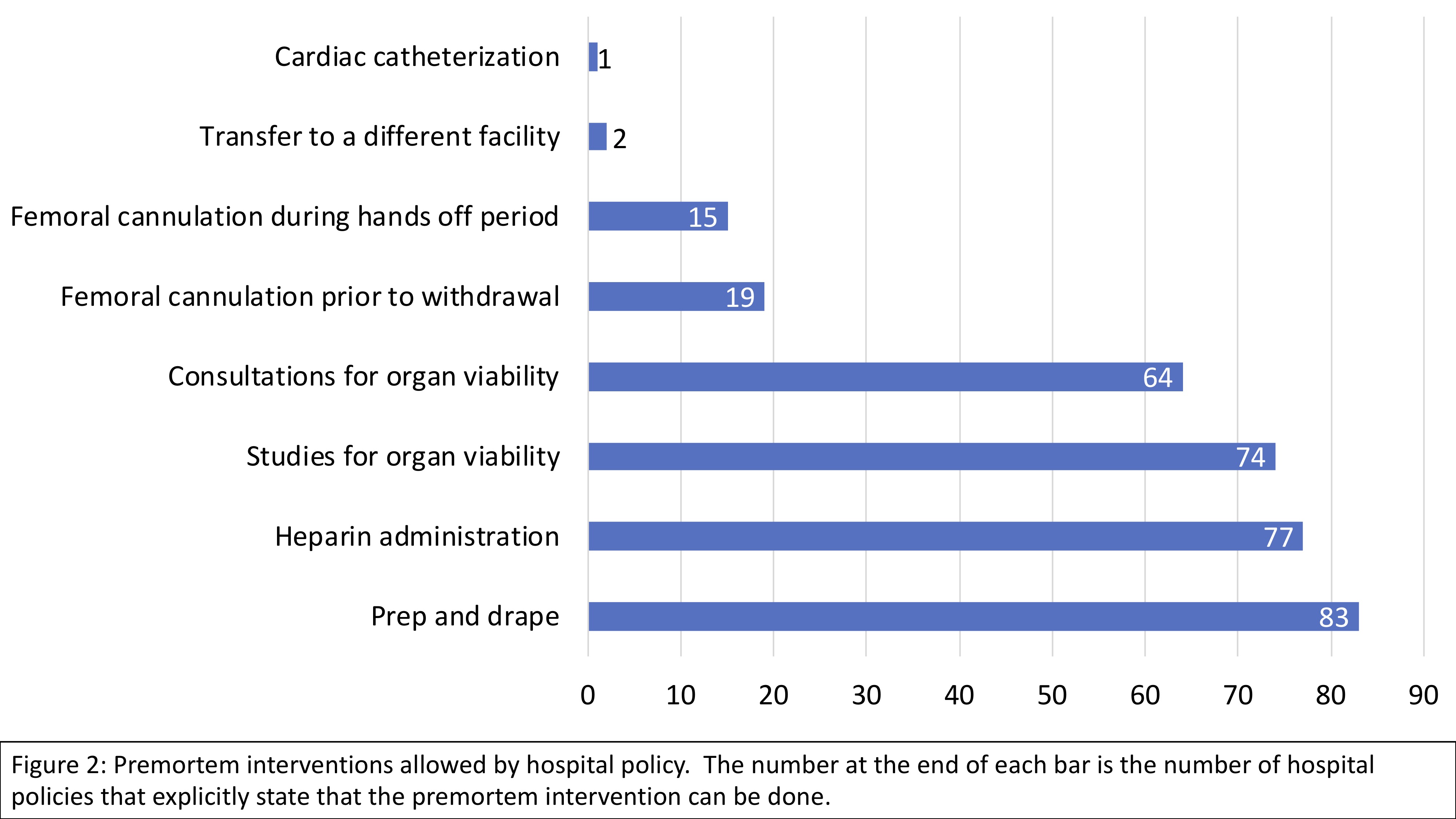
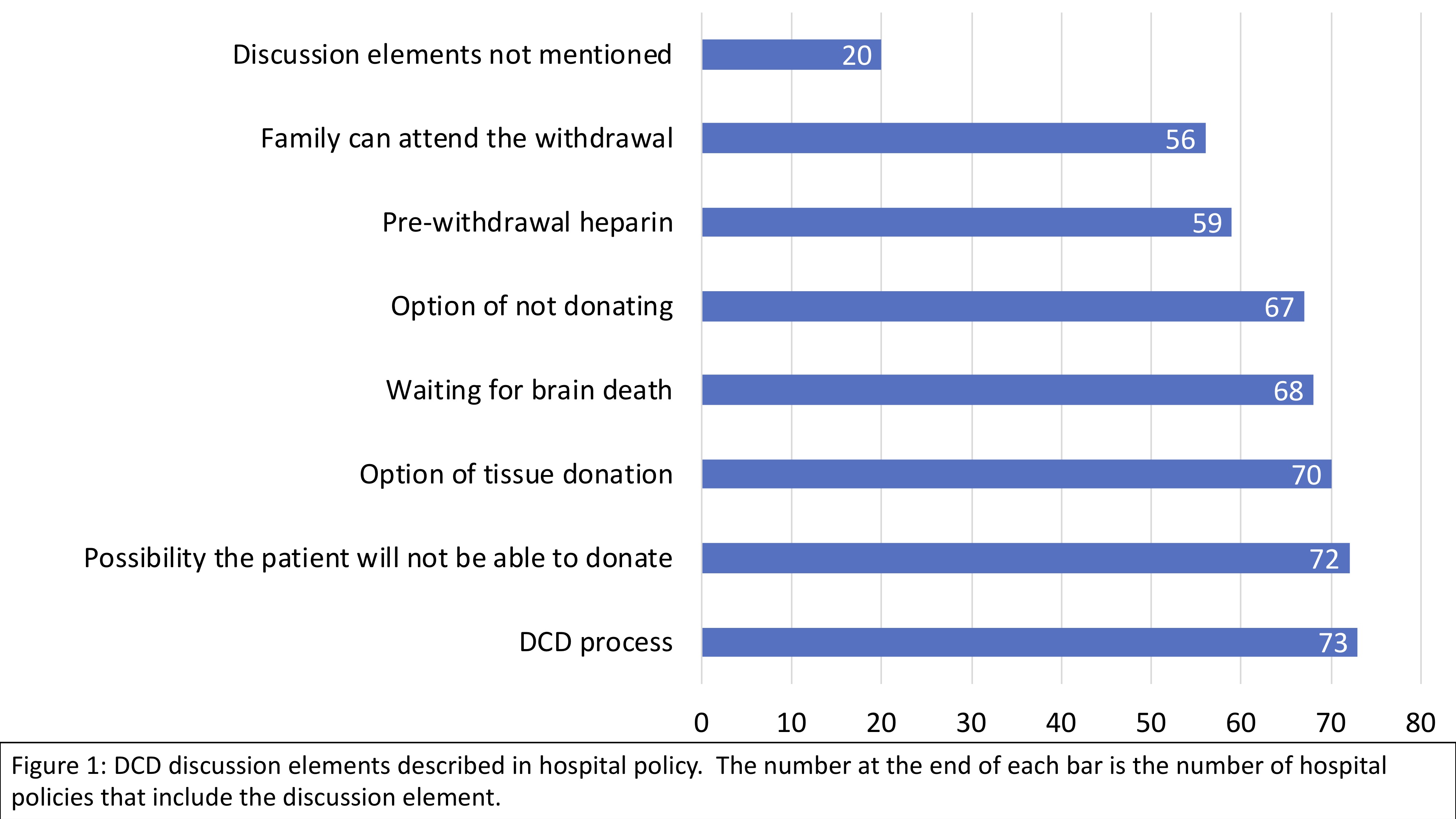
*Results: 1911 DCD donor referrals were made from 82 hospitals, all of which had a DCD policy. The median number of DCD donors referred per hospital was 5.5 (IQR= 18) and DCD donors who completed donation per hospital was 1 (IQR = 4) (Table 1). Many polices were missing elements of the DCD process. 17.4% policies do not designate OPO as a point of referral while 7.2% policies do not specify time for OPO contact. 8.2% policies do not specify who could authorize donation. 20.4% do not specify discussion elements. 10.2% do not state whether or not family members can be present. 22.5% do not specify a time limit from withdrawal to death. (Figure 1). There was variability in premortem interventions with 84.69% of policies allowing for prepping and draping but only 1.02% of policies allowing cardiac catherization prior to withdrawal of life sustaining treatment. (Figure 2).
*Conclusions: We found variation in DCD policy elements including allowance of pre-mortem interventions, OR time limit, and the location of withdrawal. It is imperative develop best practice guidelines to decrease variability in DCD policies given the increasing number of DCD donors and increasingly complex procurement operations with multiple surgical teams.
| Yes (n) | % | No (n) | % | |
| Transplant center | 9 | 9.18 | 89 | 90.82 |
| Systempolicy | 40 | 40.82 | 58 | 59.18 |
| Transfers donors | 4 | 4.08 | 82 | 83.67 |
| Referred ≥ 1 DCD | 82 | 83.67 | 16 | 16.33 |
| Completed ≥ 1 DCD | 60 | 61.22 | 38 | 38.78 |
To cite this abstract in AMA style:
Shabbir R, Chebrolu S, Vines E, Trahan C, Niles P, Testa G, Wall A. Variation Exists in Hospital Policies for Donation After Circulatory Death Within a Single Donor Service Area [abstract]. Am J Transplant. 2022; 22 (suppl 3). https://atcmeetingabstracts.com/abstract/variation-exists-in-hospital-policies-for-donation-after-circulatory-death-within-a-single-donor-service-area/. Accessed May 28, 2026.« Back to 2022 American Transplant Congress