Three-Month Pancreas Graft Function Significantly Influences Survival Following Simultaneous Pancreas-Kidney Transplantation in Type 2 Diabetes
1Washington University in St. Louis, St. Louis
2University of Colorado, Denver
3Johns Hopkins University, Baltimore
4Saint Louis University, St. Louis.
Meeting: 2018 American Transplant Congress
Abstract number: A357
Keywords: Outcome, Pancreas transplantation
Session Information
Session Name: Poster Session A: Pancreas and Islet: All Topics
Session Type: Poster Session
Date: Saturday, June 2, 2018
Session Time: 5:30pm-7:30pm
 Presentation Time: 5:30pm-7:30pm
Presentation Time: 5:30pm-7:30pm
Location: Hall 4EF
A successful simultaneous pancreas-kidney transplantation (SPK) may improve quality of life, reduce the progression of diabetic complications, and possibly prolong patient and kidney allograft survival compared to kidney transplant alone in patients with type 1 diabetes. However, the use of SPK as a transplant option in patients with type 2 diabetes (T2DM) and severe kidney disease remains limited.
We examined Organ Procurement and Transplantation Network (OPTN) data for patients with T2DM who received decreased donor kidney transplant alone (DD_KA, n=27987), living donor kidney transplant alone (LD_KA, n=13583), or SPK (n=831) between 2000 and 2016. Among the SPK recipients, 14% (n=119) had pancreas failure within 3 months of transplant (SPK,-P) and 86% (n=712) had a functional pancreas (SPK,P+). Associations of transplant type with all cause graft failure and patient death (adjusted hazard ratio, 95% LCL aHR 95% UCL) were quantified by multivariate Cox regression including adjustment for recipient, donor, and transplant factors.
Among kidney transplant recipients with T2DM, only 2% received SPK. SPK recipients were more likely to be young (age < 50), lean (body mass index < 30 kg/m2), and less likely to have zero HLA mismatches. Compared to SPK, P+, recipients of DD_KA (aHR 1.451.802.24, aHR 1.942.543.33) and LD_KA (aHR 1.061.321.65, aHR 1.381.822.39) had a significant higher risk of graft failure and death, respectively. However, patient with SPK, P- had the highest risk of graft failure (aHR 3.695.578.41) and patient death (6.5810.2515.95). 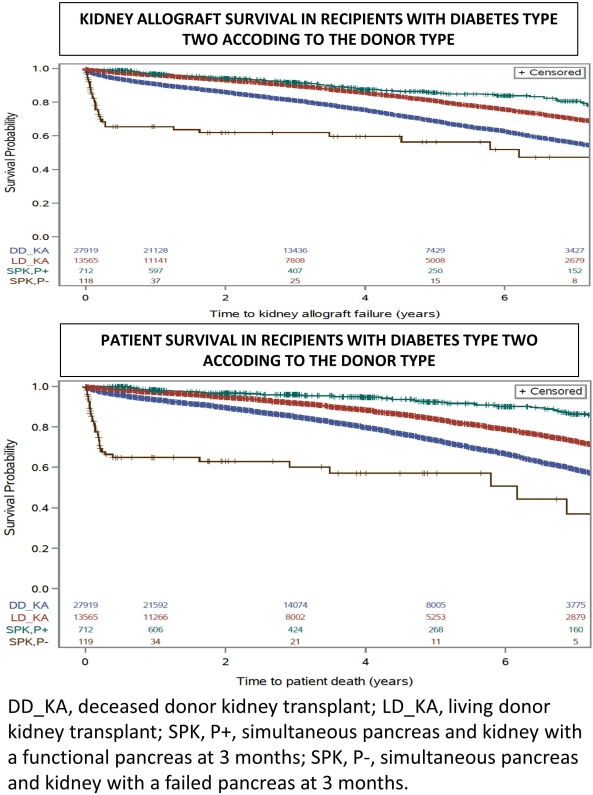
SPK recipients with functioning pancreas grafts at 3 months had superior outcomes compared to LD_KT and DD_KT. However, in 14% of the case of SPK, failed pancreas provides the worst outcome. Further studies are warranted to decrease technical failure of pancreas graft at 3 months.
CITATION INFORMATION: Alhamad T., Kunjal R., Malone A., Brennan D., Wiseman A., Wellen J., Hicks V., Lentine K. Three-Month Pancreas Graft Function Significantly Influences Survival Following Simultaneous Pancreas-Kidney Transplantation in Type 2 Diabetes Am J Transplant. 2017;17 (suppl 3).
To cite this abstract in AMA style:
Alhamad T, Kunjal R, Malone A, Brennan D, Wiseman A, Wellen J, Hicks V, Lentine K. Three-Month Pancreas Graft Function Significantly Influences Survival Following Simultaneous Pancreas-Kidney Transplantation in Type 2 Diabetes [abstract]. https://atcmeetingabstracts.com/abstract/three-month-pancreas-graft-function-significantly-influences-survival-following-simultaneous-pancreas-kidney-transplantation-in-type-2-diabetes/. Accessed May 17, 2026.« Back to 2018 American Transplant Congress