Should Renin Angiotensin Blockade Be the Mainstay of Hypertension Treatment in Kidney Donors?
U of MN, Mpls.
Meeting: 2016 American Transplant Congress
Abstract number: A121
Keywords: Donation, Hypertension, Kidney
Session Information
Session Name: Poster Session A: Kidney Donor Outcomes
Session Type: Poster Session
Date: Saturday, June 11, 2016
Session Time: 5:30pm-7:30pm
 Presentation Time: 5:30pm-7:30pm
Presentation Time: 5:30pm-7:30pm
Location: Halls C&D
Introduction: The prevalence of hypertension (HTN) in kidney donors is comparable to what is seen in the general population. How HTN in donors is treated is largely unknown. Importantly, whether renin-angiotensin-aldosteron system (RAAS) blockade offers a superior advantage over other agents is not known. The hypothesis here is that interruption of the hyperfiltration in the setting of a single kidney would be more protective than other agents that control systemic HTN but not intra-glomerular HTN.
Methods: Between 1963 and 2014, our center performed 4267 living donor nephrectomies. All donors are followed prospectively through surveys and clinic records. We determined the incidence of HTN, how it is treated (ACE vs ARB vs other anti-hypertensive) and compared renal outcomes and overall mortality in those hypertensive donors on ACE/ARB vs. others.
Results: In total, 1121 (26%) of donors developed HTN at 14.6±11.4 years from donation. Roughly half of hypertensive donors received an ACE/ARB. These donors were more likely to be diabetic (20.6% vs 11.8%, p<0.0001) and had a higher current eGFR (60.1±0.9 vs 57.7±0.8, p=0.04) but were otherwise comparable to those receiving other anti-hypertensives.
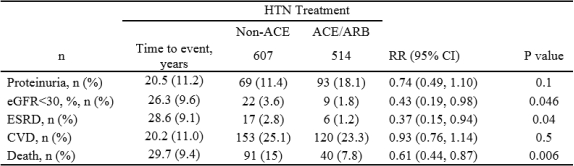
After adjusting for age, BMI, SBP, DBP, eGFR, time from donation, diabetes development after donation, any history of smoking, and eGFR at last follow-up, we found that those receiving ACE/ARB were less likely to reach an eGFR < 30 ml/min, less likely to develop ESRD and also 39% less likely to die (Table 1).
Conclusions: 1) A third of kidney donors develop HTN 2) 50% of hypertensive donors received an ACE/ARB 3) Hypertensive donors receiving ACE/ARB appear to have better GFR, less ESRD and also better survival.
These data support considering ACE/ARB as the first line therapy for hypertension in kidney donors.
CITATION INFORMATION: Sanchez O, Ferrara L, Berglund D, Reule S, Spong R, Issa N, Kukla A, Matas A, Ibrahim H. Should Renin Angiotensin Blockade Be the Mainstay of Hypertension Treatment in Kidney Donors? Am J Transplant. 2016;16 (suppl 3).
To cite this abstract in AMA style:
Sanchez O, Ferrara L, Berglund D, Reule S, Spong R, Issa N, Kukla A, Matas A, Ibrahim H. Should Renin Angiotensin Blockade Be the Mainstay of Hypertension Treatment in Kidney Donors? [abstract]. Am J Transplant. 2016; 16 (suppl 3). https://atcmeetingabstracts.com/abstract/should-renin-angiotensin-blockade-be-the-mainstay-of-hypertension-treatment-in-kidney-donors/. Accessed May 19, 2026.« Back to 2016 American Transplant Congress