Short- and Long-Term Outcomes of Mycophenolate Versus Azathioprine in a Large Cohort of Renal Transplant Recipients
1Barnes-Jewish Hospital, St. Louis
2Washington University School of Medicine, St. Louis.
Meeting: 2015 American Transplant Congress
Abstract number: 209
Keywords: Azathioprine, Immunosuppression, Mycophenolate mofetil, Rejection
Session Information
Session Name: Concurrent Session: Kidney: Immunosupression Minimization
Session Type: Concurrent Session
Date: Monday, May 4, 2015
Session Time: 2:15pm-3:45pm
 Presentation Time: 2:51pm-3:03pm
Presentation Time: 2:51pm-3:03pm
Location: Room 113-BC
Purpose: Early studies comparing mycophenolate mofetil (MMF) to azathioprine (AZA) post-renal transplantation demonstrated superiority of MMF over AZA for the prevention of acute rejection (AR). This increase in risk is not apparent among AZA treated patients also receiving tacrolimus (tac); however, long-term outcome differences have not been analyzed in a large cohort of patients. Our center utilizes AZA in place of mycophenolic acid (MPA)-containing products (MMF/enteric-coated mycophenolate sodium) due to similar AR rates and less GI toxicity with AZA. We sought to determine if antimetabolite use by age variances influenced short- and long-term outcomes in a large cohort of renal transplant recipients.
Methods: A retrospective cohort study was performed of adult renal recipients transplanted from January 1999-October 2014 who were maintained on tac and corticosteroids. Retransplanted patients were excluded. Patients were classified into groups based on age (>50) and use of AZA or MPA. The primary outcome was the incidence of AR. Secondary outcomes included the incidence of transplant glomerulopathy (TG), chronic rejection (CR), graft loss, and death.
Results: 1656 patients were included. Overall, 148 (8.9%) experienced AR. Younger patients were significantly more likely to experience AR regardless of antimetabolite used. 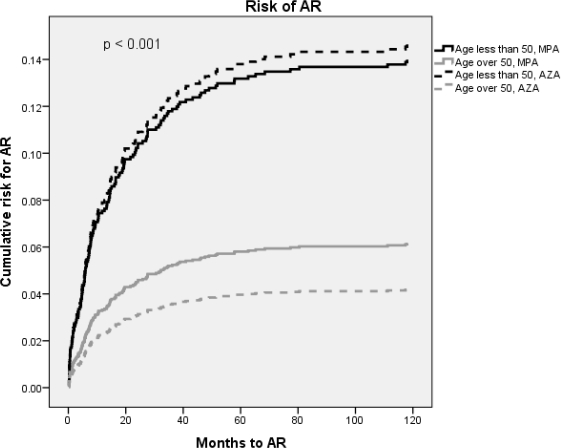 Numerically, younger patients on MPA had a higher incidence of CR and TG, but the difference was not statistically significant. More older, AZA-treated patients experienced graft loss and significantly more of them died.
Numerically, younger patients on MPA had a higher incidence of CR and TG, but the difference was not statistically significant. More older, AZA-treated patients experienced graft loss and significantly more of them died.
| Age ≤ 50, MPA N=637 | Age ≤ 50, AZA N=87 | Age > 50, MPA N=809 | Age > 50, AZA N=123 | p Value | |
| Mean age (years ± SD) | 37.8 ± 8.3 | 35.8 ± 9.2 | 60.8 ± 7.2 | 61 ± 6.9 | <0.001 |
| Caucasian race (%) | 66.9 | 74.7 | 73.1 | 78.9 | 0.444 |
| AR (%) | 13 | 13.8 | 5.9 | 4.1 | <0.001 |
| CR (%) | 2.7 | 1.1 | 1.6 | 0.8 | 0.338 |
| TG (%) | 3.5 | 2.3 | 2.7 | 2.4 | 0.813 |
| Graft loss (%) | 14.3 | 13.8 | 15.6 | 23.6 | 0.072 |
| Death (%) | 3.8 | 5.7 | 11.4 | 21.1 | <0.001 |
Conclusions: There is no difference in the incidence of short- or long-term outcomes between AZA or MPA. Younger patients had a higher incidence of AR regardless of antimetabolite used.
To cite this abstract in AMA style:
Bowman L, Horwedel T, Hagopian J, Brennan D. Short- and Long-Term Outcomes of Mycophenolate Versus Azathioprine in a Large Cohort of Renal Transplant Recipients [abstract]. Am J Transplant. 2015; 15 (suppl 3). https://atcmeetingabstracts.com/abstract/short-and-long-term-outcomes-of-mycophenolate-versus-azathioprine-in-a-large-cohort-of-renal-transplant-recipients/. Accessed June 3, 2026.« Back to 2015 American Transplant Congress