Real World Data Support International Consenus Guidelines on Management of CMV after Kidney Transplantation
Oslo University Hospital - Rikshospitalet, Oslo, Norway
Meeting: 2019 American Transplant Congress
Abstract number: B230
Keywords: Cytomeglovirus, Ganciclovir, Kidney transplantation, Prophylaxis
Session Information
Session Name: Poster Session B: Kidney Infections
Session Type: Poster Session
Date: Sunday, June 2, 2019
Session Time: 6:00pm-7:00pm
 Presentation Time: 6:00pm-7:00pm
Presentation Time: 6:00pm-7:00pm
Location: Hall C & D
*Purpose: Cytomegalovirus (CMV) naïve kidney transplant recipients (R-) transplanted with an organ from a CMV positive donor (D+) are at high risk for CMV disease. For the D+R- recipients the updated TTS International Consensus Guidelines on CMV Management depicts no preference with regard to prophylactic or preemptive preventive approach, provided an adequate surveillance of CMV PCR when the preemptive approach is used. Our center switched from a preemptive approach, with active surveillance, to routinely 6 month valganciclovir (vGCV) prophylaxis in 2011. Whether the long-term outcomes are different with these alternate strategies is not known.
*Methods: Altogether, complete national data from 410 D+R- kidney transplant recipients were available (2007-2010; 151 recipients with active surveillance receiving preemptive vGCV therapy vs. 2011-2017; 260 recipients whom received vGCV prophylaxis from time of engraftment; 900 mg once daily, adjusted for renal function). All 1660 R+ kidney transplant recipients in the period 2007-2017 served as controls for the effect of the two time era. Long-term graft and patient outcomes were retrieved from the Norwegian Renal Registry. All patients have given written informed consent for use of their data.
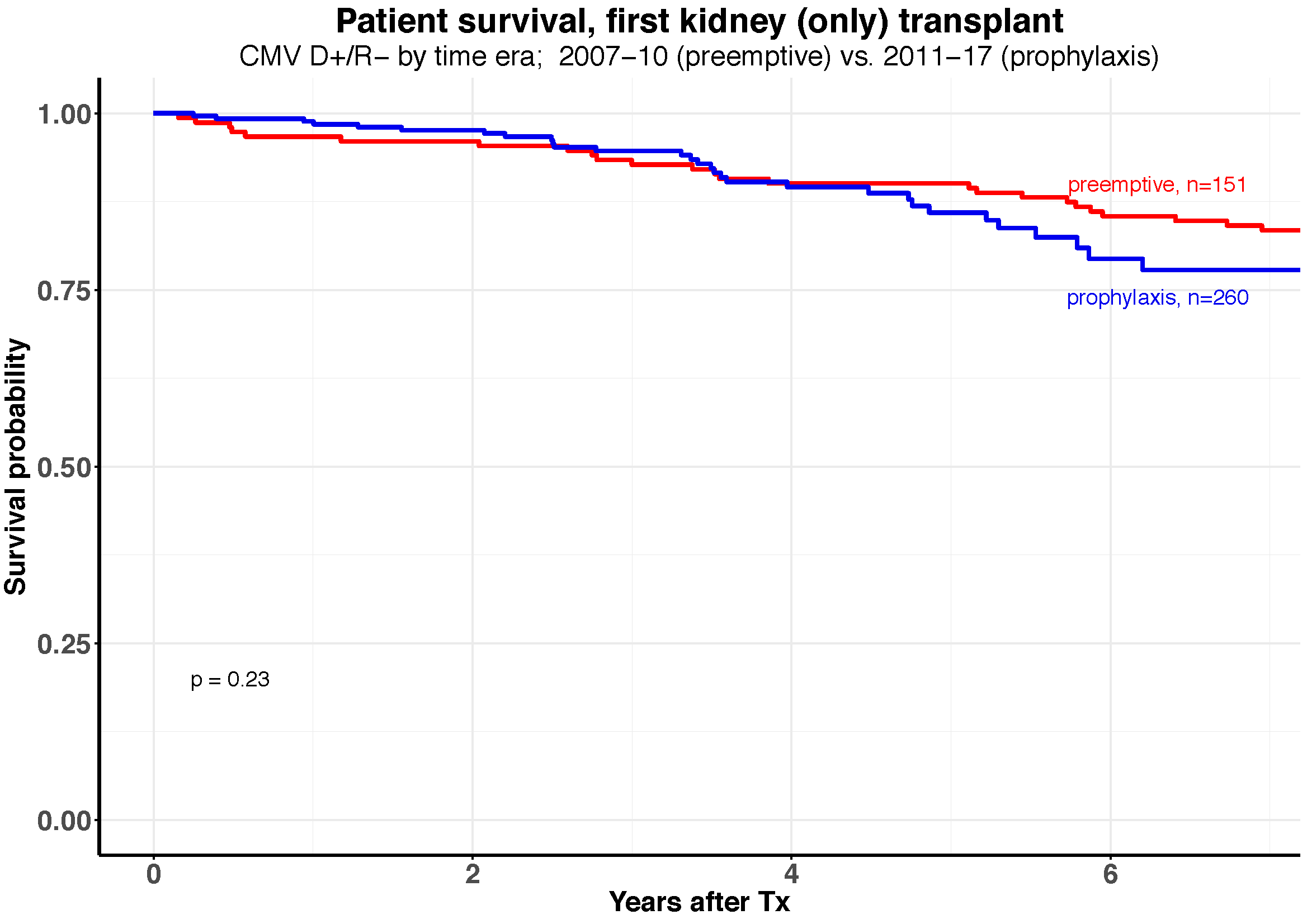
*Results: The actuarial 5 years patient survival in D+R- patients was not different with preemptive compared with prophylaxis treatment; preemptive 89% [95% CI: 85%-95%] vs. prophylactic 86% [81%-92%] (Figure 1, P=0.23). Also, the crude and death censored graft survival were similar; 85% [80%-90%] vs. 77% [71%-84%] (P=0.13) and 92% [88%-97%] vs. 87% [82%-93%] (P=0.29), respectively. In R+ patients the corresponding 5 years patient and death censored graft survival rates remained unchanged in the two time eras; 86% [83%-88%] vs. 86% [83%-88%] (P=0.69) and 93% [91%-95%] vs. 93% [91%-95%] (P=0.77), respectively.
*Conclusions: The long-term outcomes of preemptive therapy or prophylaxis for CMV prevention in high-risk kidney transplant recipients were similar. These “real world” findings support the international consensus guidelines which recommend the use of either strategy as preferred by the different transplant centers.
To cite this abstract in AMA style:
Asberg A, Kro GB, Reisæter AV, Hartmann A, Midtvedt K. Real World Data Support International Consenus Guidelines on Management of CMV after Kidney Transplantation [abstract]. Am J Transplant. 2019; 19 (suppl 3). https://atcmeetingabstracts.com/abstract/real-world-data-support-international-consenus-guidelines-on-management-of-cmv-after-kidney-transplantation/. Accessed March 27, 2026.« Back to 2019 American Transplant Congress