Preoperative Blood Pressure and Risk of Delayed Graft Function in Deceased Donor Kidney Transplantation
University of Pittsburgh Medical Center, Pittsburgh, PA
Meeting: 2022 American Transplant Congress
Abstract number: 776
Keywords: Effector mechanisms, Kidney transplantation, Obesity, Post-operative complications
Topic: Clinical Science » Kidney » 35 - Kidney: Cardiovascular and Metabolic Complications
Session Information
Session Name: Kidney: Cardiovascular and Metabolic Complications
Session Type: Poster Abstract
Date: Saturday, June 4, 2022
Session Time: 5:30pm-7:00pm
 Presentation Time: 5:30pm-7:00pm
Presentation Time: 5:30pm-7:00pm
Location: Hynes Halls C & D
*Purpose: Evaluate association between preoperative blood pressure and delayed graft function (DGF) in deceased donor kidney transplantation (DDKT)
*Methods: In this single center study of adult DDKT recipients transplanted between 2015-2019, we evaluated if preoperative mean arterial pressure (MAP) affected risk of DGF using multivariable logistic regression that adjusted for donor and recipient factors, cold ischemia time and receipt of preoperative hemodialysis. DGF was defined as need for dialysis within the first week. Preoperative MAP was obtained by averaging the first blood pressure reading after hospital admission and the last reading prior to being transferred to the surgical holding area. Pre-emptive transplant recipients were excluded. We also investigated if the risk of DGF was moderated by donation after circulatory death (DCD) status, recipient diabetes, BMI and use of anti-hypertensive medications. For recipient characteristics associated with increased DGF risk and preoperative MAP, we performed a mediation analysis to estimate the degree of DGF risk mediated through preoperative MAP.
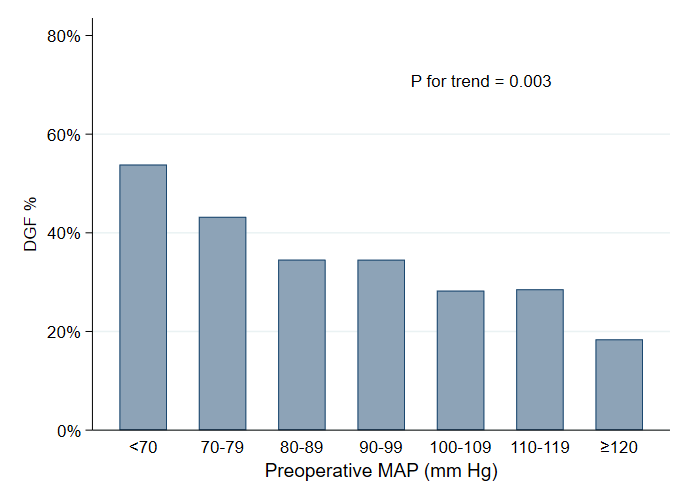
*Results: Among 562 deceased donor kidney recipients, 178 patients (31.7%) experienced DGF with median DGF duration of 4 days (interquartile range 1-9). Preoperative MAP was lower among patients with DGF than those without DGF (97 vs 102 mm of Hg; p=0.001). When DGF risk was evaluated across categories of preoperative MAP, risk of DGF decreased with increasing preoperative MAPs (p for trend = 0.003). This trend was present even among patients with blood pressures in the normotensive and hypertensive range.
There was a 2% lower risk for DGF for each 1mm of Hg increase in MAP, on both univariable (OR 0.98; 95% CI 0.97-0.99, p=0.001) and multivariable analysis (OR 0.98 per mm Hg; 95% CI 0.96-0.99; p=0.01). This increased risk was similar with no statistically significant interaction effect between perioperative MAP and donor (donation after circulatory death) and recipient characteristics (diabetes, body mass index and use if of antihypertensive medications). Preoperative MAP was negativity correlated with recipient BMI and duration of pre transplant dialysis. On mediation analysis, MAP accounted for 12% and 16% of the DGF risk associated with recipient BMI and pre-transplant dialysis duration respectively.
*Conclusions: In DDKT, DGF incidence increased as preoperative MAP decreased, even among those without hypotension. MAP negatively correlated with recipient BMI and dialysis duration and mediated some of the increased DGF risk from obesity and long dialysis vintage.
To cite this abstract in AMA style:
Wazir S, Abbas M, Ratanasreemehta P, Zhang C, Puttarajappa CM. Preoperative Blood Pressure and Risk of Delayed Graft Function in Deceased Donor Kidney Transplantation [abstract]. Am J Transplant. 2022; 22 (suppl 3). https://atcmeetingabstracts.com/abstract/preoperative-blood-pressure-and-risk-of-delayed-graft-function-in-deceased-donor-kidney-transplantation/. Accessed May 19, 2026.« Back to 2022 American Transplant Congress