Patient and Graft Survival in Pediatric Renal Transplant Recipients Compared to Adult Multi-Organ (Kidney-Pancreas, Simultaneous Liver-Kidney, or Heart-Kidney) Transplant Recipients: An Analysis of OPTN Data
1CPSST Departments of Surgery and Renal Transplantation, Driscoll Children's Hospital, Corpus Christi, TX
2UNOS, Richmond, VA.
Meeting: 2018 American Transplant Congress
Abstract number: B218
Keywords: Kidney transplantation, Multivisceral transplantation, Pediatric, Survival
Session Information
Session Name: Poster Session B: Kidney: Pediatrics
Session Type: Poster Session
Date: Sunday, June 3, 2018
Session Time: 6:00pm-7:00pm
 Presentation Time: 6:00pm-7:00pm
Presentation Time: 6:00pm-7:00pm
Location: Hall 4EF
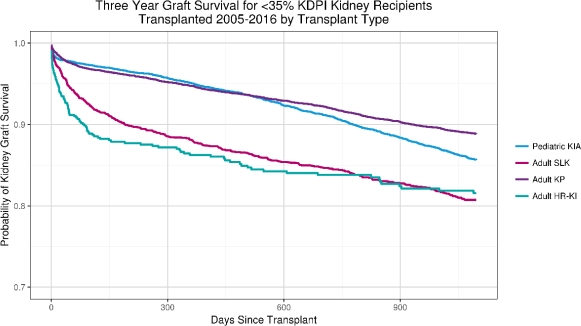
Under the current kidney allocation system (KAS), pediatric (PED) renal transplant (RTx) candidates have a priority to kidneys from donors with KDPI <35%. However, multi-organ (MOTx) adult candidates have priority over children who are candidates for kidney alone (KIA) Tx . We hypothesized that kidney graft survival (K-GS) and patient survival (PS) in PED KIA Tx recipients is superior to those of adult MOTx. We analyzed OPTN data for RTx from 2005 to 2016. We analyzed 3-year PS and K-GS for PED KIA Tx recipients and for adult kidney-pancreas (KP), simultaneous liver-kidney (SLK), and heart-kidney (HR-KI) Tx using log-rank tests. For KDPI <35% donors, PS was superior in PED KIA Tx compared to adult KP, SLK, and HR-KI (p<0.0001) [Figure 1], and K-GS was superior in PED KIA Tx compared to adult SLK and HR-KI (p<0.0001), but lower than adult KP (p<0.0001).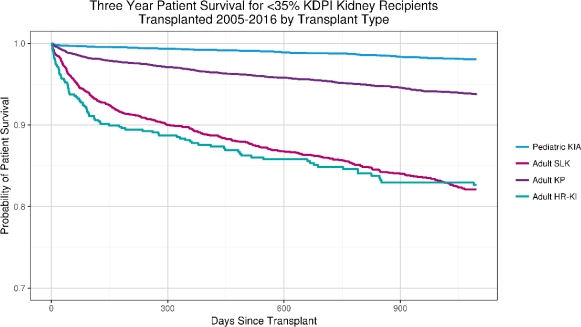
 For KDPI 35-85% donors, PED KIA Tx had superior PS compared to all other MOTx (p<0.0001), and also superior K-GS compared to adult SLK (P<0.0001) and HR-KI (p=0.008, multiple comparisons adjusted p=0.0769), but inferior to adult KP (p=0.008, adjusted p=0.0105). In conclusion, PED KIA Tx patients have better PS compared to adult KP, SLK, and HR-KI patients regardless of donor KDPI, and better K-GS except when compared to adult KP Tx. The inferior PS in adult MOTx recipients is most likely related to non-renal co-morbidities, however, the reasons for decreased K-GS in PED KIA Tx compared to KP Tx are unclear and need further study. We speculate non-adherence in adolescent patients, recurrent disease, and technical issues in younger patients may account for decreased GS compared to adult KP Tx recipients.
For KDPI 35-85% donors, PED KIA Tx had superior PS compared to all other MOTx (p<0.0001), and also superior K-GS compared to adult SLK (P<0.0001) and HR-KI (p=0.008, multiple comparisons adjusted p=0.0769), but inferior to adult KP (p=0.008, adjusted p=0.0105). In conclusion, PED KIA Tx patients have better PS compared to adult KP, SLK, and HR-KI patients regardless of donor KDPI, and better K-GS except when compared to adult KP Tx. The inferior PS in adult MOTx recipients is most likely related to non-renal co-morbidities, however, the reasons for decreased K-GS in PED KIA Tx compared to KP Tx are unclear and need further study. We speculate non-adherence in adolescent patients, recurrent disease, and technical issues in younger patients may account for decreased GS compared to adult KP Tx recipients.
CITATION INFORMATION: Almond P., Al-Akash S., Stewart D., Robinson A. Patient and Graft Survival in Pediatric Renal Transplant Recipients Compared to Adult Multi-Organ (Kidney-Pancreas, Simultaneous Liver-Kidney, or Heart-Kidney) Transplant Recipients: An Analysis of OPTN Data Am J Transplant. 2017;17 (suppl 3).
To cite this abstract in AMA style:
Almond P, Al-Akash S, Stewart D, Robinson A. Patient and Graft Survival in Pediatric Renal Transplant Recipients Compared to Adult Multi-Organ (Kidney-Pancreas, Simultaneous Liver-Kidney, or Heart-Kidney) Transplant Recipients: An Analysis of OPTN Data [abstract]. https://atcmeetingabstracts.com/abstract/patient-and-graft-survival-in-pediatric-renal-transplant-recipients-compared-to-adult-multi-organ-kidney-pancreas-simultaneous-liver-kidney-or-heart-kidney-transplant-recipients-an-analysis-of-op/. Accessed May 15, 2026.« Back to 2018 American Transplant Congress