Outcomes of Adult Dual Kidney Transplants by KDRI in the United States
Department of Surgery, Albert Einstein College of Medicine, Bronx
Department of Medicine, University of Florida, Gainesville
Meeting: 2013 American Transplant Congress
Abstract number: D1756
Background: Current UNOS guidelines do not provide adequate discrimination of kidneys that should be transplanted as single versus dual. To better define selection of kidneys for dual transplantation (DKT) we evaluated the utility of the kidney donor risk index (KDRI) to define kidneys with better outcomes when transplanted as DKT. Methods: Using US registry data from 1995 to 2010 of de novo KTX recipients of adult deceased-donor kidneys we examined overall patient and graft survival of single and dual kidney recipients stratified by KDRI group ≤1.4 (n=49,294), 1.41-1.8 (n=15,674), 1.8-2.2 (n=6,523), and > 2.2 (n=2,791). Survival distributions were examined using the Kaplan Meier method and comparison of survival times between single and dual groups were conducted using the log rank test. Multivariate analysis was conducted using Cox Proportional Hazards regression with the following variables: age, gender, race, cause of end-stage renal disease, body mass index, dialysis duration, peak panel reactive antibody, HLA mismatch, cold ischemia time, machine perfusion, insurance type, and transplant year Results: On Kaplan-Meier analysis DKT was associated with a graft survival advantage for KDRI > 2.2 (p=0.017) (Figure 1), but not KDRI ≤1.4, 1.4-1.8, or 1.8-2.2 (NS).
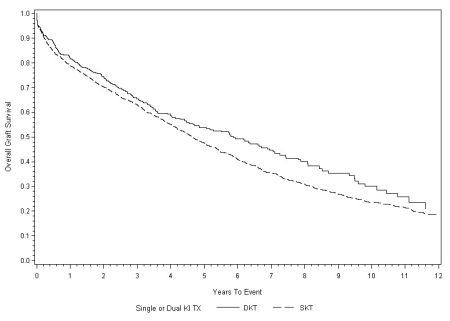
On multivariate analysis, the use of DKT for kidneys with KDRI > 2.2 was associated with a significant benefit in terms of overall graft survival [adjusted hazard ratio (aHR) 0.83, 95% confidence interval (CI) 0.72-0.96] and death-censored graft survival (aHR 0.80, 95%CI 0.66-0.98) compared to transplantation of single kidneys within the same KDRI group. There was no graft survival benefit with the use of DKT with kidneys from donors with KDRI ≤1.4 (aHR 0.94, CI 0.70-1.26), KDRI 1.4-1.8 (aHR 0.99, CI 0.84-1.17), or KDRI 1.8-2.2 (aHR 0.91, CI 0.79-1.06). There were no significant differences in patient survival with the use of DKT versus SKT in each of the four KDRI groups. Conclusions: KDRI is a useful discriminatory tool for the determination of graft survival benefit with the use of dual kidney transplantation.
To cite this abstract in AMA style:
Klair T, Gregg A, Kayler L. Outcomes of Adult Dual Kidney Transplants by KDRI in the United States [abstract]. Am J Transplant. 2013; 13 (suppl 5). https://atcmeetingabstracts.com/abstract/outcomes-of-adult-dual-kidney-transplants-by-kdri-in-the-united-states/. Accessed May 24, 2026.« Back to 2013 American Transplant Congress