Liver Retransplantation and Renal Failure: The Benefit of Simultaneous Kidney Transplant
1Department of Surgery, University of California San Diego, San Diego, CA
2Department of Medicine, University of California San Diego, San Diego, CA.
Meeting: 2018 American Transplant Congress
Abstract number: A233
Keywords: Kidney/liver transplantation, Liver transplantation, Renal failure, Retransplantation
Session Information
Session Name: Poster Session A: Liver Retransplantation and Other Complications
Session Type: Poster Session
Date: Saturday, June 2, 2018
Session Time: 5:30pm-7:30pm
 Presentation Time: 5:30pm-7:30pm
Presentation Time: 5:30pm-7:30pm
Location: Hall 4EF
Liver retransplantation has poor survival compared to primary liver transplant. Renal failure is a proven negative risk factor for survival with retransplant. Our aim was to evaluate renal failure in liver retransplant to determine what factors may impact survival and any benefit of simultaneous kidney transplant.
From March 1st 1994 to December 31st 2016 there were 78,218 primary liver transplants and 4460 retransplants after removal of exceptions (status 1 and patients < 18 years old) in the UNOS database. 703 of these retransplants received a simultaneous liver and kidney transplant (SLK). Kidney disease was defined as a glomerular filtration rate (GFR) less than 30 or the need for dialysis.
Patients who underwent SLK were significantly older than those undergoing liver retransplant alone with a longer time from previous liver transplant (2571 days vs 1530), lower GFR at transplant (75.1 vs 35.6) and lower body mass index (25.8 kg/m2 vs 25.3). 56.9% were on dialysis versus 11.8% who did not receive a kidney. They also received significantly lower donor risk index donors (1.290 vs 1.258).
Our findings demonstrate significantly worse survival in patients undergoing liver retransplantation with kidney disease (80.4% 1-year, 65.6% 5-year survival vs. 67.6%/50.1% (p < 0.005)). Patients with kidney disease who received SLK had a survival curve similar to those without kidney disease undergoing liver retransplantation alone (78.4% 1-year, 64.9% 5-year survival (p=0.527)). 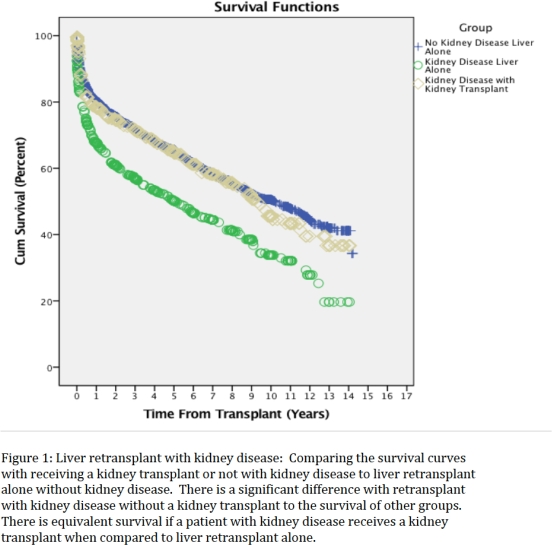 There was no observed survival benefit to SLK with a GFR above 30.
There was no observed survival benefit to SLK with a GFR above 30.
In conclusion, we found significant survival benefit to receiving SLK for patients on dialysis or with a GFR less than 30. The survival curve for SLK patients approaches that of patients without kidney disease undergoing only liver retransplant. At a GFR above 30 we did not see a benefit to SLK. Further research is needed to evaluate if different guidelines should exist for SLK at retransplantation given the poorer overall survival of liver retransplantation when compared to primary liver transplant.
CITATION INFORMATION: Berumen J., Irine V., Mita S., Gabriel S., Kristin M. Liver Retransplantation and Renal Failure: The Benefit of Simultaneous Kidney Transplant Am J Transplant. 2017;17 (suppl 3).
To cite this abstract in AMA style:
Berumen J, Irine V, Mita S, Gabriel S, Kristin M. Liver Retransplantation and Renal Failure: The Benefit of Simultaneous Kidney Transplant [abstract]. https://atcmeetingabstracts.com/abstract/liver-retransplantation-and-renal-failure-the-benefit-of-simultaneous-kidney-transplant/. Accessed March 29, 2026.« Back to 2018 American Transplant Congress