Liver May Not Protect Against Kidney Rejection in Simultaneous Liver-Kidney Transplantation (SLK), The
Northwestern University Feinberg School of Medicine, Chicago, IL
Meeting: 2013 American Transplant Congress
Abstract number: D1694
Introduction: Due to the parallel liver transplant, SLK recipients are thought to be protected from kidney rejection and receive similar immunosuppression (IS) as liver transplant alone (LTA). However, data to support this assumption and practice are not available.
Aim: To characterize the incidence and outcomes of rejection after SLK and compare outcomes and IS requirements to LTA.
Methods: All SLK recipients from 1996-2010 were included. A more recent SLK and LTA cohort (2007-10) given identical IS regimens were matched by age, transplant year, and liver disease.
Results: 181 received SLK: age 54.0 ± 10.8 years, 60.9 % male, 32.0 % HCV+. One year patient, liver, and kidney graft survival were 82.9%, 80.7% and 79.6 %, respectively. Kidney rejection occurred in 14.3%: 20 (11.0%) acute cellular (ACR), 4 (2.2%) antibody-mediated, and 2 (1.1%) chronic rejection (CR). Liver rejection occurred in 16.1%: 22 (12.2%) ACR and 7 (3.9%) CR. Graft failure (5 kidney, 4 liver) contributed to 9 (25.8%) deaths. Within 5 years, 7 (3.9%) required hemodialysis and 5 (2.8%) required an SLK or LTA retransplant. For the SLK and LTA cohorts (n=36 each), age, gender, comorbidities, liver function, mean CNI doses/troughs, and two year patient/graft survival were similar. While more SLKs were on ≥ 2 IS agents (76.5% vs. 48.3% p=0.02) and on higher MPA doses (645.9 ± 530.1 vs. 321.8 ± 626.4 mg/day; p=0.03), eGFR was lower (53.4 ± 30.9 vs. 69.6 ± 19.4 ml/min; p=0.02) at 2 years. The eGFR difference was primarily due to the SLK subset on only 1 IS agent.
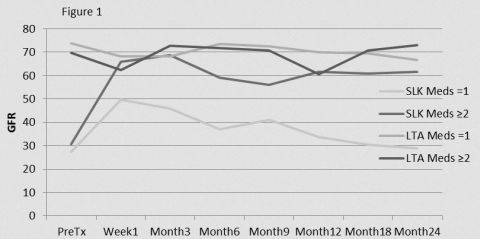
Multivariate analysis revealed that SLK itself (p<0.001) and SLK with IS monotherapy (p=0.049) were the only predictors of declining eGFR.
Conclusions: A high incidence (14.3%) of kidney rejection occurred in our large SLK population, indicating that the liver may not protect against kidney rejection. Monotherapy IS was associated with worse eGFR, implying that lower IS may lead to kidney graft injury in SLK. We propose that SLK IS be more similar to kidney alone than LTA to preserve renal function, although studies of protocol kidney biopsies in SLK would help elucidate the mechanisms of graft injury.
To cite this abstract in AMA style:
Krupp J, Nilles K, Gallon L, Levitsky J. Liver May Not Protect Against Kidney Rejection in Simultaneous Liver-Kidney Transplantation (SLK), The [abstract]. Am J Transplant. 2013; 13 (suppl 5). https://atcmeetingabstracts.com/abstract/liver-may-not-protect-against-kidney-rejection-in-simultaneous-liver-kidney-transplantation-slk-the/. Accessed May 24, 2026.« Back to 2013 American Transplant Congress