Learning Curve of Laparoscopic Donor Nephrectomy for Abdominal Transplant Surgery Fellows.
1Surgery, Univ. of Minnesota, Minneapolis, MN
2Biostatistics, Masonic Cancer Center, Minneapolis, MN
3Biostatistics, Univ. of Minnesota, Minneapolis, MN.
Meeting: 2016 American Transplant Congress
Abstract number: 125
Keywords: Donation, Kidney, Laparoscopy, Nephrectomy
Session Information
Session Name: Concurrent Session: Kidney Donor Surgery and Outcomes
Session Type: Concurrent Session
Date: Sunday, June 12, 2016
Session Time: 4:30pm-6:00pm
 Presentation Time: 4:30pm-4:42pm
Presentation Time: 4:30pm-4:42pm
Location: Ballroom B
PURPOSE: Laparoscopic donor nephrectomy (LDN) requires a high degree of surgical competence and skill. UNOS recommends that fellowship-trained surgeons participate in 15 LDN to be considered proficient. However, evaluating proficiency among transplant surgery fellows (TSF) in the modern training paradigm has yet to be defined.
METHODOLOGY: A retrospective intraoperative case analysis was performed to create a learning curve model (LCM). Between January 2000 and December 2010, 20 novice TSF (nTSF) rotated on the donor service of an ASTS-approved abdominal transplant surgery fellowship program. The measure of surgical performance was composed of 3 variables: 1) intraoperative time, 2) estimated blood loss, and 3) an ordinal intraoperative complication scale. For comparison, performance of graduating TSF (gTSF) was analyzed and used to score nTSF performance. Case complexity was defined by metrics obtained from donors with BMI>30, prior abdominal surgeries, renal vasculature multiplicity, and in whom a right nephrectomy was performed. Scores were tabulated in a general linear model, adjusting for case complexity and prior institutional- and TSF-accrued case volume.
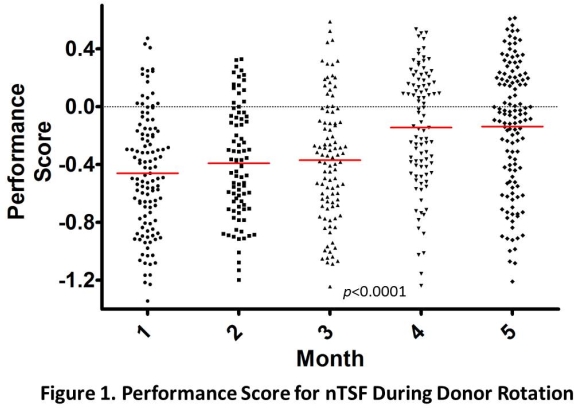
RESULTS: We estimated nTSF performance in 643 LDN. According to our LCM, BMI>30, multiple renal arteries, and prior abdominal surgeries lowered the expected performance score (EPS), while accruing institutional and TSF experience and performing a right nephrectomy raised the EPS. nTSF performance scores are depicted in Figure 1. Based on the LCM results, nTSF peak performance was achieved at the end of the third training month. This translated into an average of 24+8 cases [IQR: 22-29].
CONCLUSION: Defining the learning curve of LDN during fellowship training has critical implications for surgical education, patient safety, and program credentialing. In the current era, where fundamental laparoscopy skills are mandated during residency training, TSF seem to acquire peak LDN performance in about 24 cases.
CITATION INFORMATION: Serrano O, Bangdiwala A, Vock D, Kirchner V, Dunn T, Finger E, Pruett T, Matas A, Kandaswamy R. Learning Curve of Laparoscopic Donor Nephrectomy for Abdominal Transplant Surgery Fellows. Am J Transplant. 2016;16 (suppl 3).
To cite this abstract in AMA style:
Serrano O, Bangdiwala A, Vock D, Kirchner V, Dunn T, Finger E, Pruett T, Matas A, Kandaswamy R. Learning Curve of Laparoscopic Donor Nephrectomy for Abdominal Transplant Surgery Fellows. [abstract]. Am J Transplant. 2016; 16 (suppl 3). https://atcmeetingabstracts.com/abstract/learning-curve-of-laparoscopic-donor-nephrectomy-for-abdominal-transplant-surgery-fellows/. Accessed May 24, 2026.« Back to 2016 American Transplant Congress