Intensive Blood Pressure Control Preserves Kidney Allograft Function
1Transplant Institute, Beth Israel Deaconess Medical Center, Boston, MA, 2Biostatistics consultant, Boston, MA, 3Beth Israel Deaconess Medical Center, Boston, MA
Meeting: 2021 American Transplant Congress
Abstract number: 71
Keywords: Hypertension, Kidney transplantation, Outcome, Proteinuria
Topic: Clinical Science » Kidney » Kidney: Cardiovascular and Metabolic Complications
Session Information
Session Name: Kidney: Cardiovascular and Metabolic Complications
Session Type: Rapid Fire Oral Abstract
Date: Saturday, June 5, 2021
Session Time: 6:00pm-7:00pm
 Presentation Time: 6:20pm-6:25pm
Presentation Time: 6:20pm-6:25pm
Location: Virtual
*Purpose: Kidney transplant recipients (KTRs) are at higher risk of major adverse cardiovascular events compared to the general population, with HTN being a crucial risk factor. BP targets for KTRs remain elusive. The 2009 KDIGO target of SBP<130 was based on studies in CKD population. The SPRINT trial, adopted by AHA, showed lower mortality with an intensive SBP goal (<130). We studied the effect of intensive BP control in KTRs.
*Methods: This retrospective cohort analysis included adult KTRs performed between 1/1/2002-12/31/2015 at a single academic center. BP, serum creatinine and urine protein-creatinine ratio (UPCR) were followed at 3-month intervals for 5 years after kidney transplant. Patients were divided into 3 groups based on their mean SBP (mmHg): <=120, 121-130 and >130. eGFR was calculated at 12 and 60 months using the MDRD equation. Primary outcomes were patient survival, graft survival and an eGFR decline of 25% or greater in the 5 years of follow up. Graft failure was defined as new diagnosis of ESRD post-transplant. Comparison of categorical variables was done using Pearson Chi2 test and continuous variables using Kruskal Wallis H test. Patient and graft survival were studied using Kaplan Meier survival analysis.
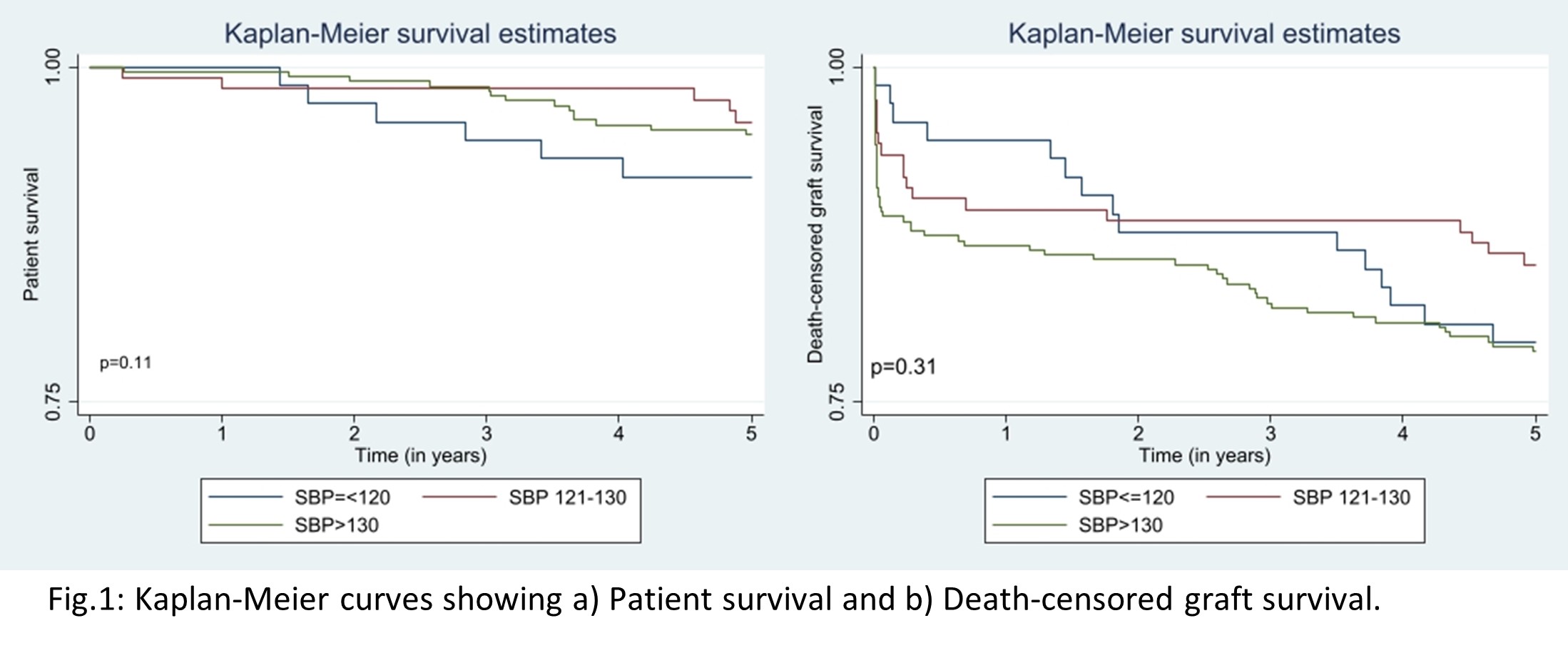
*Results: Table 1 & 2. Patients with mean SBP 121-130 had better patient and graft survival (Fig 1). Higher proportion of patients with SBP>130 suffered a decline of 25% or greater in their GFR and had a UPCR>1g/g during the 5-year follow-up as compared to those with SBP<=130 (Table 2).
*Conclusions: In this cohort, most patients had average SBP>130. We show that a SBP of 121-130 mmHg is associated with improved patient and graft survival compared both to higher (>130) or lower (<=120) mean values as well as slower decline of renal allograft function.
| Total (n=473) | SBP<=120 (n=73) | SBP 121-130 (n=122) | SBP>130 (n=278) | p-value | |
| Males | 295 (62.4%) | 33 (45.2%) | 75 (61.5%) | 187 (67.3%) | 0.002 |
| Age in years (mean, min-max) | 52.9 (23-82) | 47.7 (29-69) | 51.8 (23-82) | 54.9 (25-78) | 0.0001 |
| Mean SBP (mmHg) | 134 +/- 13.9 | 113.7 +/- 5.7 | 125.7 +/- 2.7 | 142.9 +/- 9.9 | 0.0001 |
| Mean DBP (mmHg) | 76.6 +/- 9.7 | 72.3 +/- 5.9 | 74.9 +/- 8.0 | 78.5 +/- 10.6 | 0.0001 |
| Mean eGFR at 12mo (mL/min) | 51.5 +/- 18.4 | 55.3 +/- 20.3 | 53.9 +/- 18.6 | 49.5 +/- 17.5 | 0.0065 |
| Mean eGFR at 60mo (mL/min) | 51.8 +/- 21.5 | 55.5 +/- 20.8 | 54.8 +/- 20.9 | 49.4 +/- 21.7 | 0.014 |
| Total (n=473) | SBP<=120 (n=73) | SBP 121-130 (n=122) | SBP>130 (n=278) | p-value | |
| Patients with eGFR decline >=25% | 15.9% | 11.9% | 12.2% | 18.8% | 0.22 |
| Spot UPCR<0.5g/g | 74.3% | 81.5% | 82% | 69.4% | 0.025 |
| Spot UPCR 0.5-0.9g/g | 9.5% | 3% | 9% | 11.2% | 0.025 |
| Spot UPCR >=1g/g | 16.2% | 15.4% | 9% | 19.4% | 0.025 |
To cite this abstract in AMA style:
Agarwal KA, Agarwal UK, Silva GS, Pollick KJ, Pavlakis M. Intensive Blood Pressure Control Preserves Kidney Allograft Function [abstract]. Am J Transplant. 2021; 21 (suppl 3). https://atcmeetingabstracts.com/abstract/intensive-blood-pressure-control-preserves-kidney-allograft-function/. Accessed May 20, 2026.« Back to 2021 American Transplant Congress