Increased Survival Benefit Amongst Highest Priority Candidates Undergoing Heart Transplant Following the New Us Heart Allocation System
1Pritzker School of Medicine, University of Chicago, Chicago, IL, 2Department of Medicine, Section of Pulmonary and Critical Care Medicine, University of Chicago, Chicago, IL
Meeting: 2022 American Transplant Congress
Abstract number: 453
Keywords: Economics, Organ Selection/Allocation, Public policy, Waiting lists
Topic: Clinical Science » Ethics » 23 - Non-Organ Specific: Economics & Ethics
Session Information
Session Name: Psychosocial and Treatment Adherence
Session Type: Rapid Fire Oral Abstract
Date: Tuesday, June 7, 2022
Session Time: 3:30pm-5:00pm
 Presentation Time: 4:50pm-5:00pm
Presentation Time: 4:50pm-5:00pm
Location: Hynes Room 311
*Purpose: A key policy change in the new US heart allocation system was splitting the previous highest status (1A) into statuses 1, 2, and 3 to better stratify high acuity patients. We determined if the highest priority candidates under this new system had higher survival benefit from transplantation compared with the highest priority candidates in the prior policy.
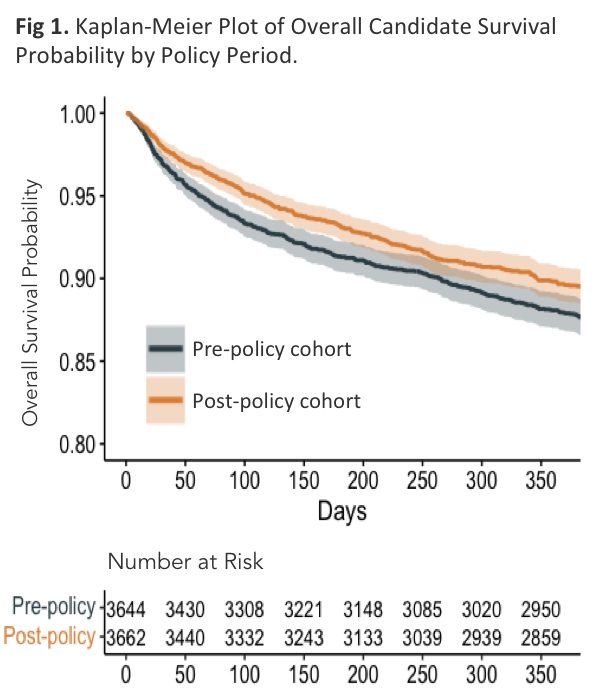
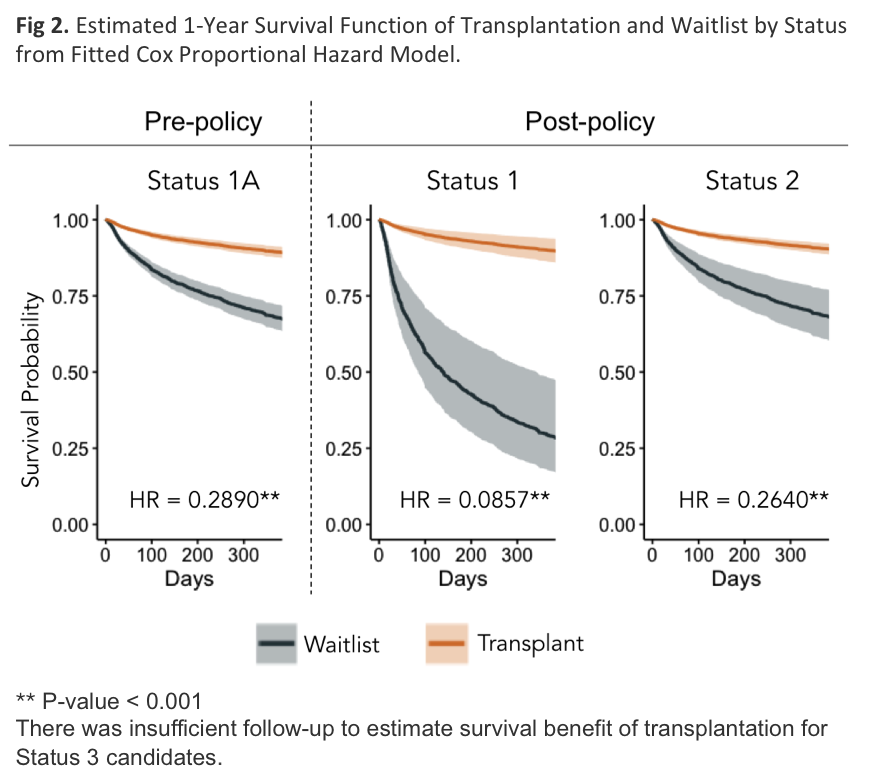
*Methods: We collected Scientific Registry of Transplant Recipients data on all adult heart transplant candidates listed in seasonally matched pre (2016-2017) and post-policy (2018-2019) cohorts. We used the Kaplan-Meier method to estimate overall survival probability amongst all candidates in both policy periods. We fitted a Cox proportional hazards model treating transplant and status as time-dependent covariates to estimate hazard ratios of transplant for each status level. Using these hazard ratios and a non-parametric Nelson-Aalen estimate of the baseline hazard, we estimated 1-year survival curves with and without transplantation.
*Results: There were 3,644 candidates listed in the pre-policy and 3,662 in the post-policy cohort. Post-policy candidates were more likely to be transplanted than those in the pre-policy cohort (66 v 60%, p<0.01) and more likely to be alive (89.7 v 88.0%, p=0.02, Fig 1) at one year. There were no statistically significant differences between cohorts in demographics or hemodynamics. Transplantation for Status 1 recipients improved absolute 1-year survival by 60.7%, a significantly greater survival benefit than the 21.4% improvement for Status 1A recipients in the pre-policy period (HR 0.086 v 0.289, p<0.01, Fig 2). The survival benefit for Status 2 recipients was similar to Status 1A recipients, improving absolute survival by 21.9% (HR 0.264 v 0.289, p=0.68).
*Conclusions: Status 1 recipients under the new policy experience greater survival benefit from transplantation than Status 1A recipients in the previous policy. Since the policy change, more medically urgent patients are stratified into the highest priority status, without significantly compromising post-transplant survival.
To cite this abstract in AMA style:
Tolmie S, Parker W. Increased Survival Benefit Amongst Highest Priority Candidates Undergoing Heart Transplant Following the New Us Heart Allocation System [abstract]. Am J Transplant. 2022; 22 (suppl 3). https://atcmeetingabstracts.com/abstract/increased-survival-benefit-amongst-highest-priority-candidates-undergoing-heart-transplant-following-the-new-us-heart-allocation-system/. Accessed May 24, 2026.« Back to 2022 American Transplant Congress