Increased Ratio of Estimated Spleen/Graft Volume Is a Strong Predictor of Posttransplant Portal Hypertension in Adult-To-Adult Living Donor Liver Transplantation: Significance of Splenectomy On Portal Venous Pressure and Patient Survival
Hepatobiliary-Pancreatic and Transplant Surgery, Mie University, Tsu, Mie, Japan.
Meeting: 2015 American Transplant Congress
Abstract number: 400
Keywords: Living-related liver donors
Session Information
Session Name: Concurrent Session: Liver: Living Donors and Partial Grafts
Session Type: Concurrent Session
Date: Tuesday, May 5, 2015
Session Time: 2:15pm-3:45pm
 Presentation Time: 2:39pm-2:51pm
Presentation Time: 2:39pm-2:51pm
Location: Room 115-AB
Splenectomy is generally performed to control portal venous pressure (PVP) in adult-to-adult living donor liver transplantation (ALDLT) with small-for-size graft. However, we sometimes experience portal hypertension after LDLT, even if graft weight to recipient weight ratio (GRWR) is more than 0.8. We investigated preoperative predicting factors affecting portal hypertension in ALDLT.
Between March 2002 to March 2013, 75 ALDLTs were performed and PVP was examined at Mie University. 56 patients of them had preoperative CT images to evaluate spleen volume. Splenectomy was performed when PVP immediately after reflow was more than 20 mmHg. In study I (75 patients), we examined initial PVP after reflow and final PVP before abdominal closure with or without splenectomy, and patient survival was evaluated. In study II (56 pts), we evaluated preoperative factors contributing to initial PVP after reflow and furthermore investigated the best index to predict initial PVP of 20 mmHg or more after reflow.
In study I, 19 patients received splenectomy because initial PVP after reflow was more than 20 mmHg, of whom 16 (84.2%) had final PVP of less than 20 mmHg. Survival rate in the patients with final PVP < 20 mmHg after splenectomy was significantly higher than that of patients with final PVP of 20 mmHg or more before abdominal closure (p=0.031). 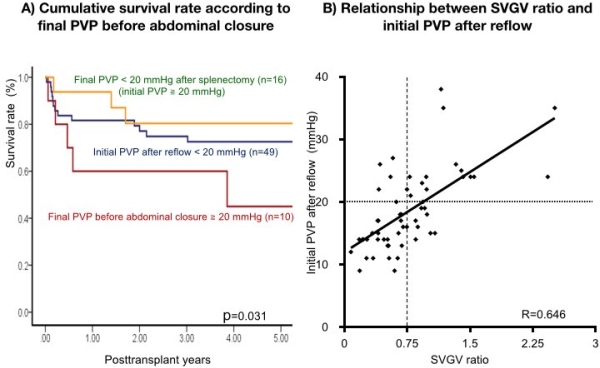 In study II, multivariable analysis revealed that estimated graft volume and spleen volume were independent factors contributing to initial PVP after reflow (p < 0.0001 and p< 0.0001, respectively). The estimated spleen to graft volume ratio (SVGVR) showed significant positive correlation with initial PVP after reflow (R=0.646, p=0.0004) and ROC analysis of SVGVR revealed that the best cut-off value for initial PVP of 20 mmHg or more after reflow was 0.75.
In study II, multivariable analysis revealed that estimated graft volume and spleen volume were independent factors contributing to initial PVP after reflow (p < 0.0001 and p< 0.0001, respectively). The estimated spleen to graft volume ratio (SVGVR) showed significant positive correlation with initial PVP after reflow (R=0.646, p=0.0004) and ROC analysis of SVGVR revealed that the best cut-off value for initial PVP of 20 mmHg or more after reflow was 0.75.
Preoperative assessment of both spleen and graft volume is very useful to predict posttransplant portal hypertension in ADLT.
To cite this abstract in AMA style:
Mizuno S, Gyoten K, Tanemura A, Murata Y, Kato H, Kuriyama N, Kishiwada M, Usui M, Sakurai H, Isaji S. Increased Ratio of Estimated Spleen/Graft Volume Is a Strong Predictor of Posttransplant Portal Hypertension in Adult-To-Adult Living Donor Liver Transplantation: Significance of Splenectomy On Portal Venous Pressure and Patient Survival [abstract]. Am J Transplant. 2015; 15 (suppl 3). https://atcmeetingabstracts.com/abstract/increased-ratio-of-estimated-spleengraft-volume-is-a-strong-predictor-of-posttransplant-portal-hypertension-in-adult-to-adult-living-donor-liver-transplantation-significance-of-splenectomy-on-portal/. Accessed May 16, 2026.« Back to 2015 American Transplant Congress