Increased Graft Survival Following Implementation of the Kidney Allocation Score
1Surgery, Duke University Hospital, Durham, NC, 2Surgery, East Carolina University, Greenville, NC
Meeting: 2020 American Transplant Congress
Abstract number: B-017
Keywords: Allocation, Graft failure, Kidney, Outcome
Session Information
Session Name: Poster Session B: Kidney Deceased Donor Allocation
Session Type: Poster Session
Date: Saturday, May 30, 2020
Session Time: 3:15pm-4:00pm
 Presentation Time: 3:30pm-4:00pm
Presentation Time: 3:30pm-4:00pm
Location: Virtual
*Purpose: The Kidney Allocation Score (KAS) was developed to improve matching of donor and recipients; we examine the effect of this change on transplantation practice and outcomes.
*Methods: Data from the UNOS STAR files was used to identify first-time adult of a deceased donor kidney-alone transplant pre-KAS (Jan 2011-Dec 2014) and post-KAS (Jan 2015-Dec 2017). Demographic variables were summarized and compared for donor and recipient. Patient and graft survival were compared by Kaplan-Meier log-rank test. Cumulative incidence function was used to estimate the probability of graft loss with death as a competing event. Follow-up was truncated to 24 months.
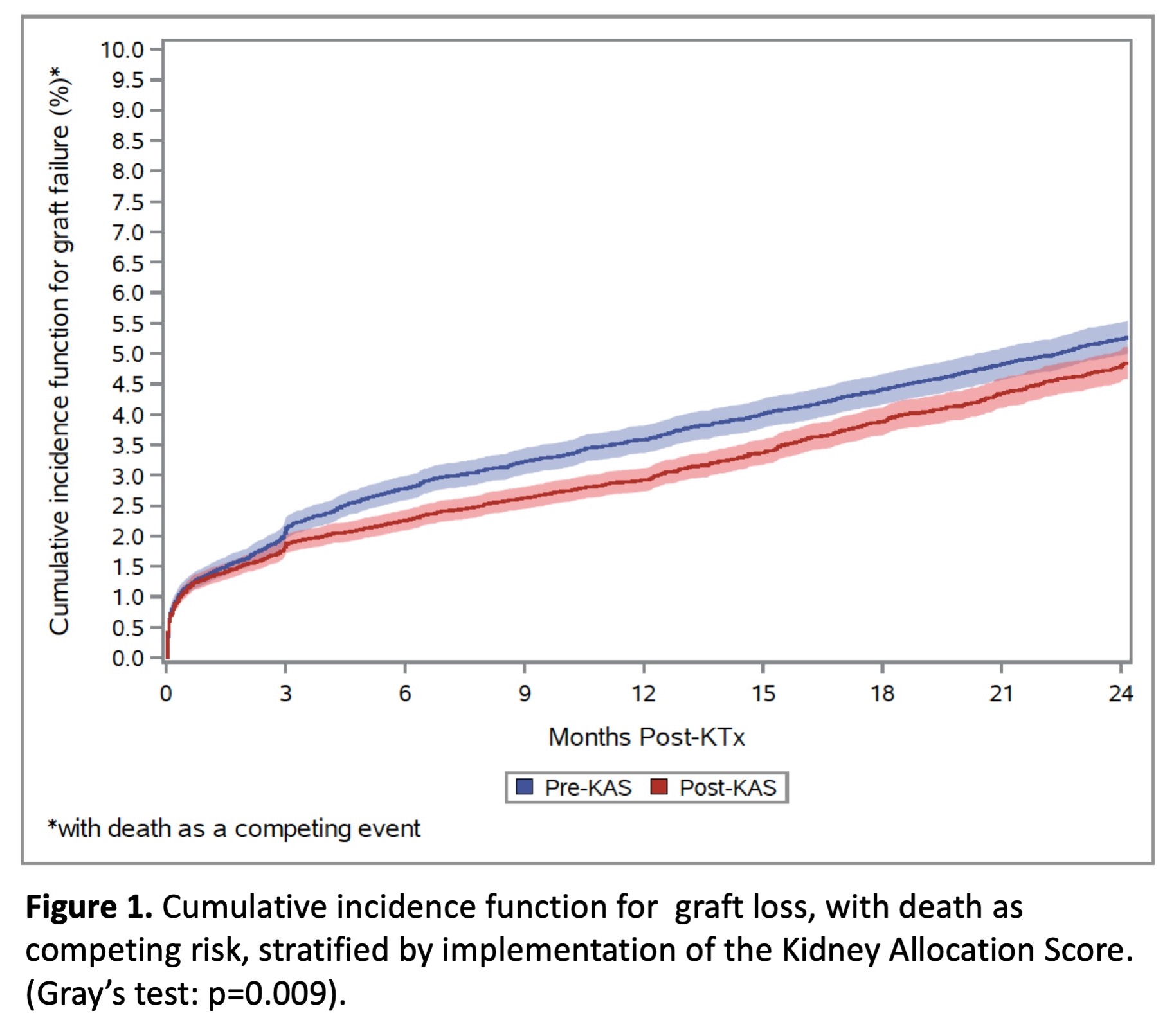
*Results: 26,612 transplants were performed pre-KAS, and 30,701 post-KAS. Compared to pre-KAS, post-KAS donors were younger, less likely to have diabetes or hypertension, and more likely to die of anoxic brain injury. Compared to pre-KAS, post-KAS gender and ethnic disparities narrowed with more female and African-American recipients. Recipients were also more likely to be diabetic, and had a higher calculated percent reactive antibody (cPRA) (Table 1). Post-KAS, kidneys were more likely to experience cold ischemia time > 24 hours (20.0% vs 18.8%, p<0.001) and to be procured after cardiac death (21.5% vs 17.8%, p<0.001). Correspondingly, post-KAS kidneys had greater delayed graft function, defined by requiring hemodialysis within the first week post-transplant (28.7% vs 26.1%, p<0.001). Patient survival did not change post-KAS (KM log rank p=0.296). Competing risks modeling demonstrated a lower hazard of graft loss post-KAS, HR 0.90 (95% CI 0.84-0.97, p=0.007). Cumulative incidence function of graft loss is presented in Figure 2.
*Conclusions: Implementation of the KAS has allowed the use of higher-quality kidneys in younger, more sensitized recipients. Despite an increase in transplants for highly sensitized recipients, KA has resulted in a 10% reduction in hazard of graft loss. Longer follow-up and attention to organ discard practices are needed to quantify the long-term impact of the KAS system.
| Pre-KAS
(n=26,612)
|
Post-KAS
(n=30,701)
|
p-value | |
| Donor age > 60, n(%) | 2,292 (8.6%) | 2,299 (7.5%) | <0.001 |
| Donor Diabetes, n(%) | 2,168 (8.2%) | 2,171 (7.1%) | <0.001 |
| Donor Cause of Death, n(%)
Anoxia
Stroke
Head Trauma
CNS Tumor
Other
|
8,632 (32.4%)
8,251 (31.0%)
8,872 (33%)
134 (0.5%)
723 (2.7%)
|
12,603 (41.1%)
7,783 (25.4%)
9,333 (30.4%)
116 (0.4%)
866 (2.8%)
|
<0.001 |
| KDPR>85%, n(%) | 2,272 (8.5%) | 2,228 (7.3%) | <0.001 |
| Recipient Age > 60, n(%) | 9,869 (37.1%) | 10,462 (34.1%) | <0.001 |
| cPRA, Mean (SD) | 16.9 (30.3) | 19.5 (33.1) | <0.001 |
| cPRA>80%, n(%) | 2,617 (9.8%) | 3,640 (11.9%) | <0.001 |
To cite this abstract in AMA style:
Samoylova ML, Shaw BI, Irish W, Kesseli SJ, Connor A, Barbas AS, McElroy L, Ravindra KV. Increased Graft Survival Following Implementation of the Kidney Allocation Score [abstract]. Am J Transplant. 2020; 20 (suppl 3). https://atcmeetingabstracts.com/abstract/increased-graft-survival-following-implementation-of-the-kidney-allocation-score/. Accessed March 26, 2026.« Back to 2020 American Transplant Congress