Impact of Community Risk on Early Hospital Readmission Following Kidney Transplant
1Surgery, Johns Hopkins University, School of Medicine, Baltimore, MD
2Epidemiology, Johns Hopkins University, School of Public Health, Baltimore, MD
3Quantitative Health Sciences, Cleveland Clinic, Cleveland, OH.
Meeting: 2015 American Transplant Congress
Abstract number: 201
Keywords: Kidney transplantation, Outcome, Risk factors
Session Information
Session Name: Concurrent Session: Kidney: Hospitalization/Readmission
Session Type: Concurrent Session
Date: Monday, May 4, 2015
Session Time: 2:15pm-3:45pm
 Presentation Time: 2:39pm-2:51pm
Presentation Time: 2:39pm-2:51pm
Location: Room 118-AB
Background: Early hospital readmission (EHR) is associated with increased morbidity, mortality, and cost in kidney transplantation (KT). Community risk may be associated with EHR above and beyond patient-level risk factors.
Methods: USRDS and SRTR data were linked with county health rankings for 40,751 adult, kidney-only transplant recipients from January 2005 through December 2011. County health rankings are assigned based on access to care, prevalence of comorbidity, environmental hazards, and behaviors of individuals within each U.S. county. Rankings range from 1-40 and were treated categorically to capture community risk: lowest risk (<10), low-intermediate risk (11-20), high-intermediate risk (21-30), and highest risk (>30). EHR was any readmission within 30 days of discharge following KT. Logistic regression was used to determine the association between community risk and EHR adjusting for patient-level risk factors.
Results: Over 50% of KT recipients were from high-intermediate risk or highest risk communities. 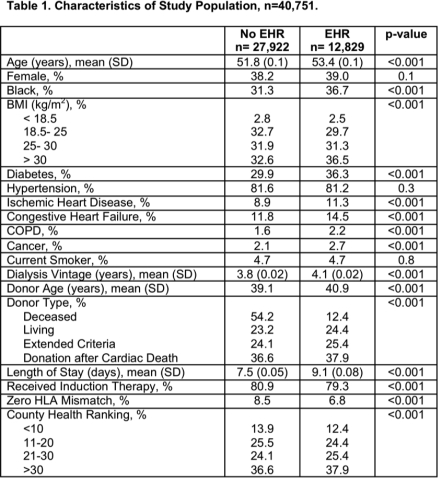 There was no statistically significant difference in EHR among KT recipients living in lowest risk or low-intermediate risk communities. The odds of EHR was statistically significantly increased for KT recipients living in a high-intermediate risk (aOR 1.13, 95% CI: 1.05-1.22, p-value= 0.001) or a highest risk community (aOR 1.11, 95% CI: 1.03- 1.19, p-value= 0.004).
There was no statistically significant difference in EHR among KT recipients living in lowest risk or low-intermediate risk communities. The odds of EHR was statistically significantly increased for KT recipients living in a high-intermediate risk (aOR 1.13, 95% CI: 1.05-1.22, p-value= 0.001) or a highest risk community (aOR 1.11, 95% CI: 1.03- 1.19, p-value= 0.004). 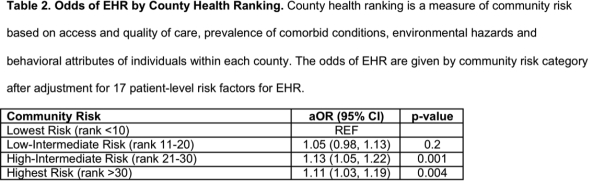
Conclusions: Over 50% of KT recipients live in high-intermediate and highest risk communities, which is associated with increased odds of EHR. Community risk should be considered by physicians working to reduce EHR following KT.
To cite this abstract in AMA style:
King E, Kucirka L, McAdams-DeMarco M, Massie A, Schold J, Segev D. Impact of Community Risk on Early Hospital Readmission Following Kidney Transplant [abstract]. Am J Transplant. 2015; 15 (suppl 3). https://atcmeetingabstracts.com/abstract/impact-of-community-risk-on-early-hospital-readmission-following-kidney-transplant/. Accessed June 2, 2026.« Back to 2015 American Transplant Congress