Impact of a Pharmacist in an Outpatient Heart Transplant Clinic
1UNC Health Care, Chapel Hill, NC, 2Eshelman School of Pharmacy, Chapel Hill, NC
Meeting: 2021 American Transplant Congress
Abstract number: 1190
Keywords: Heart transplant patients, Outcome, Outpatients, Post-operative complications
Topic: Clinical Science » Heart » Heart and VADs: All Topics
Session Information
Session Name: Heart and VADs: All Topics
Session Type: Poster Abstract
Session Date & Time: None. Available on demand.
Location: Virtual
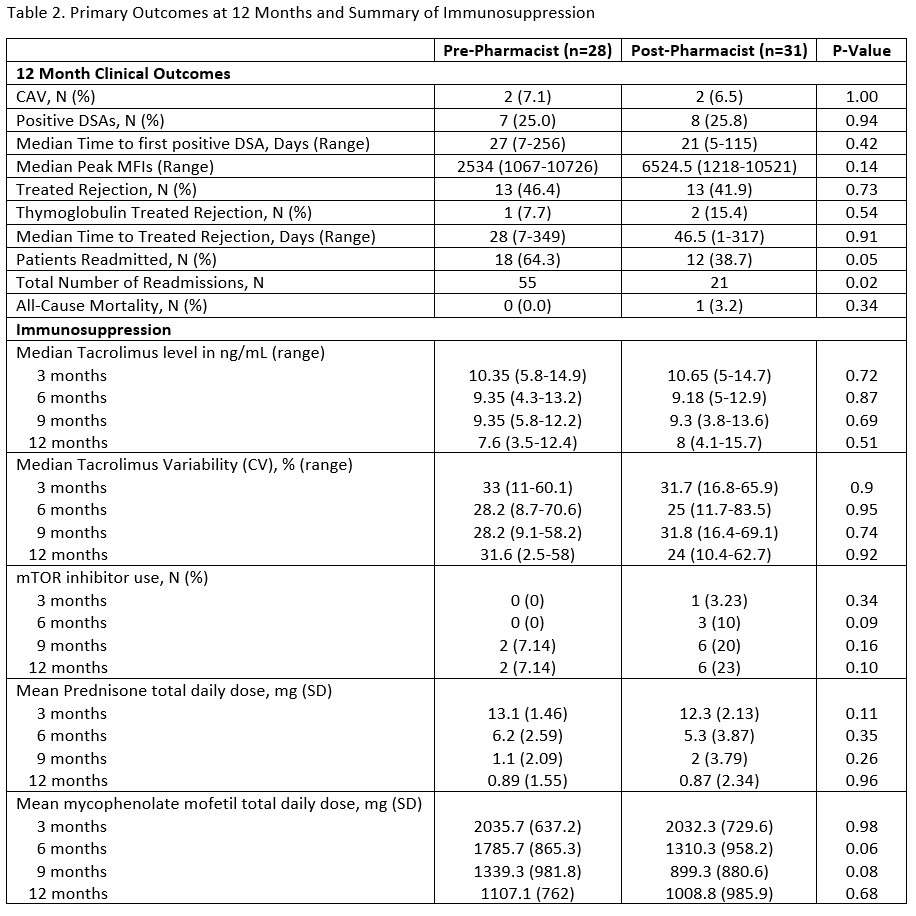
*Purpose: Data describing the impact of a pharmacist in ambulatory medication management of heart transplant recipients (HTRs) is lacking. Following the addition of an ambulatory clinical pharmacist to the heart transplant team in 1/2017 we assessed outcomes at 1 year post-transplant of HTRs seen by a pharmacist compared to those not seen by a pharmacist at a single center.
*Methods: A retrospective unpaired analysis of de novo HTRs from 1/2015-12/2019 was conducted. Dual organ, pediatric and HTRs who did not survive to discharge were excluded. Incidence of cardiac allograft vasculopathy (CAV), cellular and antibody-mediated rejection, all-cause rehospitalizations, all-cause mortality, attainment of goal blood pressure, hemoglobin A1c (A1c), tacrolimus level variability (CV) and use of aspirin and statin therapy were compared between pre and post pharmacist groups at 1 year post-transplant. No other personnel or protocol changes occurred during the study period. Chi-square and unpaired t-tests were used to conduct the analysis.
*Results: 59 HTRs were included with an average of 12.2 ± 3.5 pharmacist visits per HTR in the pharmacist group. No differences in baseline demographics (Table 1) or maintenance immunosuppression (Table 2) were identified. At 1 year, the pharmacist cohort had a higher percentage of HTRs at goal blood pressure, on a statin, and on appropriate intensity statin (Figure 1), as well as fewer HTRs with any readmission and fewer total readmissions (Table 2). No differences in 1 year A1c control, tacrolimus CV, aspirin use, CAV, donor specific antibodies (DSAs), rejection or all-cause mortality were seen.
*Conclusions: Based on this single center limited cohort study, pharmacist integration into an ambulatory heart transplant team has the potential to improve 1 year outcomes by targeting goal-directed medication therapy and reducing hospital readmissions.


To cite this abstract in AMA style:
Prom A, Ricciuti D, Newman J, Doligalski C. Impact of a Pharmacist in an Outpatient Heart Transplant Clinic [abstract]. Am J Transplant. 2021; 21 (suppl 3). https://atcmeetingabstracts.com/abstract/impact-of-a-pharmacist-in-an-outpatient-heart-transplant-clinic/. Accessed June 3, 2026.« Back to 2021 American Transplant Congress